Chapter 31 Video-Assisted Minilaparotomy Surgery for Living Donor Nephrectomy
Operation indications
VAMS living donor nephrectomy is indicated for the removal of an intact kidney with ureter from a living organ donor for transplantation into a suitable recipient with end-stage renal disease. Donors should undergo proper medical and psychosocial evaluation preoperatively per the routine of the transplantation unit. The decision to permit voluntary donation of a kidney is made after a determination that there is no complicating mental dysfunction. The donor should be healthy and free of major medical problems, such as unstable coronary anatomy, heart failure, arrhythmia, valvular disease, coagulation disorders, thromboembolic disorders, and chronic lung disease (Table 31-1). Other contraindications to donor nephrectomy include age younger than 18 years, impaired renal function, renal disease, hypertension, diabetes mellitus, body mass index (BMI) more than 35, and pregnancy. Relative contraindications include microscopic hematuria, stone disease, and an abnormal kidney. In general, a history of multiple previous abdominal procedures is not a contraindication for VAMS donor nephrectomy because a retroperitoneal approach is used.
Table 31-1 Contraindications for Donor Nephrectomy, for the Donor
Preoperative evaluation, testing, and preparation
Each donor should undergo routine screening, including a medical history, physical examination, BMI determination, ABO blood typing, general biochemistry panel, hematology panel, pathogen antigen and antibody panels, 24-hour urine collection (for creatinine clearance, urinalysis, protein quantification, and culture), electrocardiogram, chest radiograph, and pregnancy testing. A donor BMI higher than 35 is a relative contraindication to donor nephrectomy, because of increased risk for postoperative donor morbidity. The glomerular filtration rate (GFR) should be 80 mL/minute or higher, or 2 standard deviations above the normal range based on age, sex, and body surface area. Donors with hypertension (blood pressure >140/90 mm Hg, as measured with ambulatory blood pressure monitoring) generally are excluded. Donors with diabetes (as defined in Table 31-1) also are excluded.
Patient positioning in the operation suite
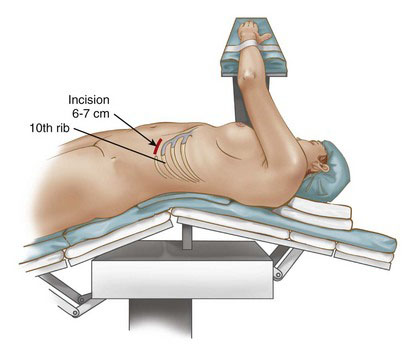
The patient is placed in the semilateral position on the operating table, as shown in Figure 31-1. The torso is positioned with the level of the kidney over the central point of bed flexion. The ipsilateral arm is fixed on an arm board, which is positioned between the upper neck and the head. A cushioning roll (viscoelastic polymer gel) is placed under the axilla. A rolled sheet is placed under the back of the patient to stabilize the torso. The contralateral leg is bent slightly, the ipsilateral leg is stretched, and a cushion is placed between the legs. The operating table then is flexed about 30 degrees at the level of the kidney. On completion of positioning, the ipsilateral shoulder will be rotated up and the hips will remain flat with respect to the table. The table flexure will have expanded the operative area between the costal margin and the iliac crest. A Foley catheter is placed. All wires, tubes, and lines are routed along the top of the operating table, near the edge. If these objects are left to fall directly off the table, then they will hinder subsequent installation of the retractors.
Positioning and placement of trocars
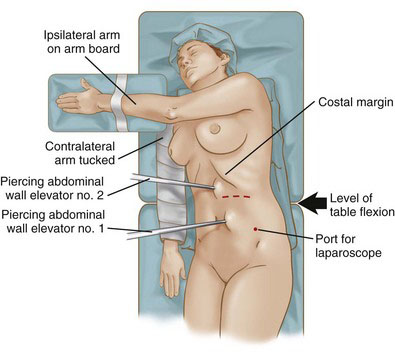
The operative space in our description of VAMS donor nephrectomy is the retroperitoneal space. In general, the operative space in a VAMS procedure is established with (1) a piercing abdominal wall elevator, (2) a piercing peritoneal (visceral) retractor, and (3) blades from an external self-retaining retractor system. The piercing abdominal wall elevator, as its name implies, enters the operative space through a separate stab incision and provides lift to the abdominal wall (Fig. 31-2). Because the operative space will be open to the atmosphere through the minilaparotomy incision, lift from abdominal wall elevator will expand this space. As described in detail later, the head of the piercing peritoneal retractor is inserted into the operative space through the minilaparotomy incision, positioned against the anteromedial abdominal wall, and held in place with an arm that pierces through the abdominal wall and is clamped to the external system.
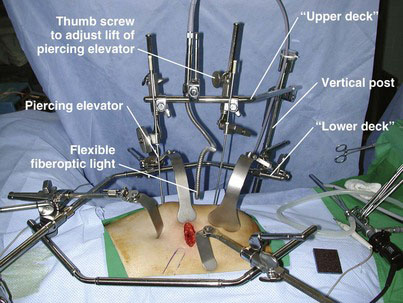
The external self-retaining retractor system we employ is a Thompson type (Thompson Surgical Instruments, Traverse City, Mich.), specifically developed for VAMS donor nephrectomy (Fig. 31-3 shows system setup; system components are shown in Fig. 31-4). This device can provide both horizontal and vertical traction simultaneously by means of its “double-decker” configuration (see Fig. 31-3). A major advantage of this configuration is that the donor nephrectomy can be performed without the need for a retracting assistant.
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


