| 14 | Vascular Malformations and Other Vascular Lesions |
 Definitions
Definitions
When describing vessel dilation in the gastrointestinal tract, the literature makes a distinction between angiodysplasia (telangiectasias) and hemangiomas. Angiodysplasia is defined as a dilation of superficial vessels while hemangiomas are defined as benign vascular tumors. However, the question as to whether the difference between the two is merely gradual and whether differentiation reflects differing pathogenesis remains unanswered.
Angiodysplasia (Telangiectasia)
 Epidemiology and Pathogenesis
Epidemiology and Pathogenesis
The pathogenesis of angiodysplasia is not entirely clear. In addition to hereditary forms, such as hereditary hemorrhagic telangiectasia (HHT), there also appear to be acquired forms, as suggested by the more frequent occurrence of angiodysplasias in the colon with increasing age. In a colonoscopic study, Richter et al. (29) found angiodysplasias in the large bowel in 1.4% of patients examined; Foutch et al. found them in 0.83 % of patients (12).
Degeneration of blood vessels. Based on pathological studies, Boley et al. (6) hypothesized that angiodysplasias in older individuals are a result of degenerative processes of the veins in the colon wall. They suggest that dilation of submucosal veins is caused by hypertrophy of the longitudinal and transverse colon musculature. Hypertrophy constricts the points of entry of the veins in the muscle layer, obstructing blood flow. Obstruction would first cause dilation of the veins surrounding the crypts and later the submucosal veins, followed by dilation of the capillaries and incompetence of the precapillary sphincters, ultimately resulting in an arteriovenous short circuit. This pathogenesis would also explain why 60-90 % of angiodysplasias are found in the right hemicolon (12, 29) where the wider lumen leads to greater wall tension (according to the Laplace law) and thus increased obstruction of venous outflow.
Ischemia. Another hypothesis suggests that angiectasias are caused by chronic ischemia. This almost certainly applies to radiation proctitis in which multiple telangiectasias are caused by mucosal ischemia.
In the pathogenesis of HHT, genetic factors are the most important determinant.
 Histology
Histology
Early-stage angiectasias present histologically as dilated, tortuous submucosal veins. Later, marked clinical presentation includes dilated veins, venoles, and capillaries with a thin lining of endothelium and a small amount of smooth muscle in the vessel wall (Fig. 14.1). Pathological changes in HHT are identical to those observed in older individuals.

Fig. 14.1 Microscopic features of angiodysplasia in the colon mucosa with hollow areas lined with endothelium (courtesy of Dr. Th. Wagner, Institute for Pathology, Augsburg Clinic).
 Clinical Course and Prognosis
Clinical Course and Prognosis
In older patients, angiodysplasia has a benign clinical course. Hemorrhage is uncommon (12,29,30), and an incidental finding during colonoscopy in a patient without a history of bleeding does not require therapy.
Telangiectasias related to HHT have a different prognosis and course. Around one-third of cases result in gastrointestinal bleeding which can be related to substantial morbidity (18, 35).
 Diagnosis
Diagnosis
 Angiectasias appear endoscopically as red, circumscribed mucosal lesions with a diameter of one millimeter to a few centimeters (
Angiectasias appear endoscopically as red, circumscribed mucosal lesions with a diameter of one millimeter to a few centimeters ( 14.1, 14.2). About half of the lesions are smaller than 5 mm (31, 38). Small angiectasias usually present as red patches with either a round, circumscribed border or a slightly irregular margin and generally are not elevated. Larger lesions usually lie above the level of the mucosa (
14.1, 14.2). About half of the lesions are smaller than 5 mm (31, 38). Small angiectasias usually present as red patches with either a round, circumscribed border or a slightly irregular margin and generally are not elevated. Larger lesions usually lie above the level of the mucosa ( 14.2 d) and have irregular borders (
14.2 d) and have irregular borders ( 14.1 b-d, 14.2a), resulting from communication with neighboring capillaries. Very large angiodysplasias have also been reported (24). Some angiodysplasias can resemble the spider naevi found in patients with liver cirrhosis (
14.1 b-d, 14.2a), resulting from communication with neighboring capillaries. Very large angiodysplasias have also been reported (24). Some angiodysplasias can resemble the spider naevi found in patients with liver cirrhosis ( 14.1 f). The number of angiodysplasias per patient can vary and the number of patients with solitary angiodysplasias is about equal to the number of those with multiple lesions (31, 38). One endoscopic study reported an average of 1.4 lesions in the colon per patient among patients with angiodysplasias (29).
14.1 f). The number of angiodysplasias per patient can vary and the number of patients with solitary angiodysplasias is about equal to the number of those with multiple lesions (31, 38). One endoscopic study reported an average of 1.4 lesions in the colon per patient among patients with angiodysplasias (29).
 14.1 Various appearances of angiodysplasias in the lower gastrointestinal tract
14.1 Various appearances of angiodysplasias in the lower gastrointestinal tract
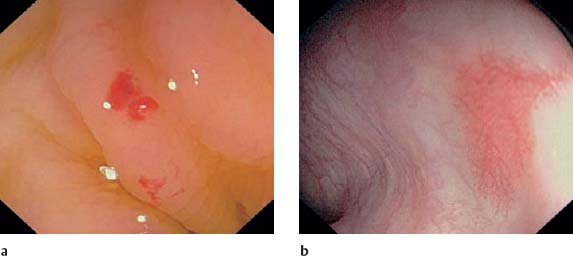
a, b Angiodysplasias in a 68-year-old man with multiple angiodysplasias in the colon and small bowel, but with no evidence of HHT. The patient was taking anticoagulants due to mitral valve endoprosthesis and had had several gastrointestinal bleeding episodes. Small angiodysplasia in the ascending colon (a). Large, patchy angiodysplasia also in the ascending colon (b).
c Angiodysplasia in the ascending colon in an older man undergoing colonoscopy due to anemia.

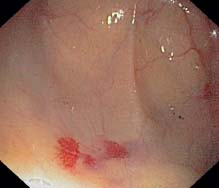
d Patchy angiodysplasia in ascending colon. Dilated and branchlike capillaries as well as a dilated vein are readily visible.

e Small angiodysplasias in ascending colon that are clearly related to discretely dilated veins.

f Spidery angiodysplasia in ascending colon with dilated vein and two dilated capillaries that are fanning out peripherally like branches.
Older patients with angiodysplasias in the colon rarely have vascular malformations in the upper gastrointestinal tract. In HHT and among patients under 50 years of age, angiodysplasias are usually distributed throughout the entire gastrointestinal tract. Thus, examination of stomach and small intestine is essential.
Endoscopic therapy
 Angiodysplasias are treated with thermocoagulation (
Angiodysplasias are treated with thermocoagulation ( 14.2). Injection of epinephrine or application of hemoclips may also be necessary if there is bleeding.
14.2). Injection of epinephrine or application of hemoclips may also be necessary if there is bleeding.
Telangiectasias in radiation proctitis. In 5-10% of patients, patients who have had radiation therapy in the pelvis develop chronic radiation injury to the rectal mucosa within 4-41 months following treatment. Endarteritis of the mucosal vessels causes both chronic mucosal ischemia and neovascularization (formation of telangiectasias).
 Identification of telangiectasias in the rectum in radiation proctitis (Figs. 14.2–14.4) is generally straightforward given localization, appearance, and patient medical history. Endoscopic appearance is characterized by a pale and vulnerable mucosa that is covered by multiple telangiectasias often extending to the anal canal (Fig. 14.5).
Identification of telangiectasias in the rectum in radiation proctitis (Figs. 14.2–14.4) is generally straightforward given localization, appearance, and patient medical history. Endoscopic appearance is characterized by a pale and vulnerable mucosa that is covered by multiple telangiectasias often extending to the anal canal (Fig. 14.5).
Endoscopic therapy
 The therapy of choice for symptomatic patients with anemia and/or blood loss is thermocoagulation using APC (Fig. 14.4).
The therapy of choice for symptomatic patients with anemia and/or blood loss is thermocoagulation using APC (Fig. 14.4).
 14.2 Thermocoagulation of angiodysplasias
14.2 Thermocoagulation of angiodysplasias
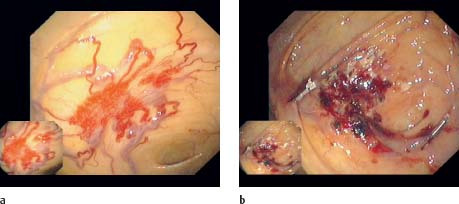
a, b Angiodysplasia in the cecum of an older woman who underwent endoscopy due to anemia. One can see dilated veins and a markedly red center formed by dilated capillaries that are branching out into the surrounding area (a). After ligation of the veins using hemoclips (Olympus) the angiodysplasia is coagulated point-by-point using APC (b).
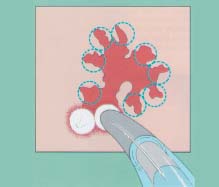
c Illustration of thermocoagulation of an angiodysplasia (based on 11). Beginning at the periphery of the angiodysplasia, one then moves toward the center. It should be taken into account that bleeding caused by coagulation may obscure vision.

d-f Patients with chronic anemia and numerous angiodysplasias in the ascending colon. An angiodysplasia, ca. 6 mm in size and slightly elevated above the mucosal surface (d). An angiodysplasia in the ascending colon (e), coagulated using APC (point coagulation) (f).

Fig. 14.2 Rectum in a female patient with prior radiation therapy for an endometrial carcinoma. One can see the pale mucosa with scattered angiodysplasias, a finding typical of late onset of radiation injury (radiation proctitis).
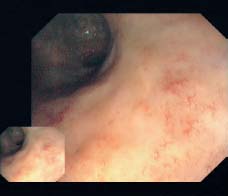
Fig. 14.3 Rectal mucosa after prior radiation therapy of an endometrial carcinoma. Tiny, newly forming vessels visible in the pale rectal mucosa.
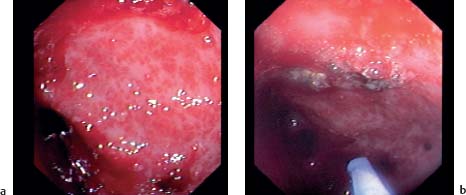
Fig. 14.4 Rectum in a patient after neoadjuvant radiation of a rectal carcinoma.
a
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


