elevated pH due to loss of CO2 from the urine
■ Specific gravity
Specific gravity is the weight of urine relative to distilled water and reflects the number and size (weight) of particles in urine. Osmolality is dependent only on the number of particles (solute concentration) in urine. Specific gravity is usually directly proportional to osmolality. However, iodinated contrast and, to a lesser extent, protein, will increase specific gravity but have little effect on osmolality. The normal range of urine specific gravity is 1.001 (very dilute) to 1.030 (very concentrated). Urine specific gravity of 1.010 is the same as plasma (isosthenuria). If specific gravity is not >1.022 after a 12-hour overnight fast (food and water), renal concentrating ability is impaired.
■ In an oliguric patient, a specific gravity >1.020 suggests normal ability to concentrate urine and prerenal failure (decreased renal blood flow), whereas ~1.010 suggests loss of tubular function (acute tubular necrosis/acute kidney injury).
■ In a hyponatremic patient, an inappropriately high specific gravity (>1.010) suggests antidiuretic hormone (ADH) secretion (see Chapter 5).
■ In a hypernatremic patient, an inappropriately low specific gravity (<1.010) suggests diabetes insipidus (central or nephrogenic) (see Chapter 5).
■ Protein
The dipstick detects primarily albumin. Normal urine has no protein by dipstick, but occasionally very concentrated urine will be trace positive for protein in healthy individuals. A positive dipstick should lead to a quantitative measurement. Classically, this was done by a 24-hour collection, but as creatinine is excreted at a constant rate, a ratio of urine albumin to creatinine or protein to creatinine is sufficient in most patients.
■ Albumin versus total protein (Shihabi et al., 1991). Healthy subjects excrete up to 30 mg of albumin and 150 to 200 mg of total protein per day (and on average 1,000 mg of creatinine per day). Thus, the normal urine albumin to creatinine ratio (UACR) is <30 mg per g and the normal urine protein to creatinine ratio (UPCR) is <150 to 200 mg per g. UACR of 30 to 300 mg per g is considered to be microalbuminuria and >300 mg per g overt albuminuria. UPCR >500 mg per g indicates overt proteinuria.
■ Classically, sulfosalicylic acid (SSA) was added to the urine to detect total protein. A discrepancy between the dipstick and SSA test (e.g., 1+ protein in dipstick and 4+ by SSA) suggested the presence of a paraprotein (e.g., myeloma protein) in the urine. A marked discrepancy between UACR and UPCR gives the same information.
■ Glucose
Normal urine does not contain glucose due to reabsorption of filtered glucose by the proximal tubule.
■ Glycosuria with elevated blood glucose—diabetes mellitus (Singer et al., 1989)
■ Glycosuria with normal blood glucose—renal glycosuria
• Isolated
• Associated with other proximal tubular dysfunction (phosphaturia, aminoaciduria, bicarbonaturia) (Fanconi syndrome). One should exclude multiple myeloma
■ Ketones
Normally, there are no ketones in the urine.
■ Ketonuria without ketoacidosis—starvation, low carbohydrate (Atkins) diet, isopropyl alcohol ingestion
■ Ketonuria with ketoacidosis—diabetic or alcoholic ketoacidosis. Note that in some patients with ketoacidosis, the dipstick may be negative due to reduction of acetoacetate to ß-hydroxybutyrate
■ Bilirubin
Normally there is no bilirubin in the urine. If present, this suggests any of the following:
■ Hepatobiliary disease (failure to conjugate and/or excrete bilirubin into the gut)
■ Hemolysis (increased production of bilirubin from heme)
■ Urobilinogen
Bilirubin is secreted in bile into the gut, where it is metabolized by microorganisms into urobilinogen. Urobilinogen is then absorbed and partially excreted into the urine. In the presence of liver disease, urobilinogen can accumulate in plasma and appear in the urine. Bilirubin without urobilinogen in the urine suggests biliary obstruction.
■ Leukocyte esterase
This is an enzyme found in white blood cells (WBCs) and indicates the presence of pyuria.
■ Urinary tract infection (UTI)
■ Sterile pyuria (see below)
■ Nitrite
Enterobacteria convert urinary nitrate to nitrite, and therefore a positive test suggests UTI. Note that not all organisms make nitrite, so UTI may be present with a negative nitrite too.
MICROSCOPIC EXAMINATION
■ RBCs
Hematuria (see Chapter 3) (Fig. 1.1)
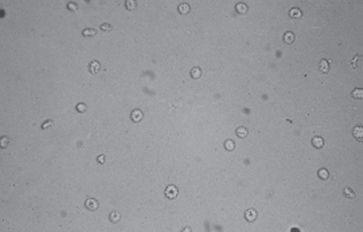
FIGURE 1.1 Red blood cells. (Image courtesy of Medcom, Inc.) (See Color Plate.)
■ WBCs
Infection (Ditchburn & Ditchburn, 1990) or sterile pyuria. With sterile pyuria, one should exclude interstitial nephritis; other causes include nonbacterial infection, prostatitis, nephrolithiasis, and glomerulonephritis. Eosinophiluria suggests interstitial nephritis (Fig. 1.2).
■ Squamous epithelial cells
Squamous epithelial cells from the skin surface or from the outer urethra can appear in urine. Their significance is that they represent possible contamination of the specimen.
■ Bacteria
Indicate possible infection (Fig. 1.3)
■ Yeast
Could be infection versus contamination. Presence of pseudomycelia suggests infection. Risk factors include indwelling catheters, recent antibiotics, immunosuppression, and diabetes.
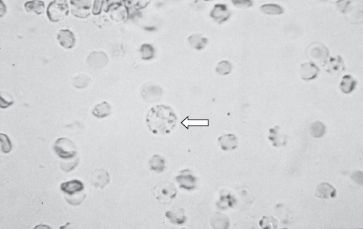
FIGURE 1.2 White blood cell (arrow). (Image courtesy of Medcom, Inc.) (See Color Plate.)
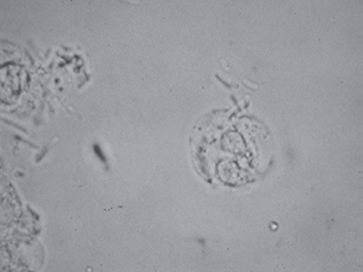
FIGURE 1.3 White blood cells and bacteria. (Image courtesy of Medcom, Inc.) (See Color Plate.)
■ Crystals
■ Calcium oxalate—dihydrate: tetragonal (envelopes); monohydrate: dumbbells—can be seen in normal urine; in large amounts, suggests calcium oxalate kidney stones or ethylene glycol poisoning (which is metabolized to oxalate) (Fig. 1.4)
■ Calcium phosphate—form in alkaline urine—amorphous; in large amounts, suggests calcium phosphate kidney stones (seen in RTA)
■ Uric acid—form in acid urine—pleomorphic, yellow/brown; when in large amounts, suggests uric acid kidney stones or nephropathy (Fig. 1.5)
■ Cystine—hexagonal—indicates cystinuria (Fig. 1.4)
■ Magnesium ammonium phosphate (triple phosphate)—coffin-lids—suggests struvite stones (a urea-splitting organism must be present to produce NH3 and elevate urine pH) (Fig. 1.6)
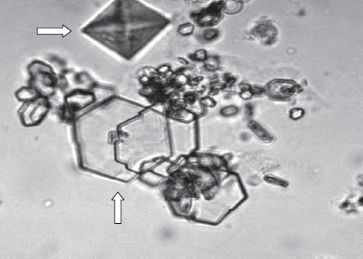
FIGURE 1.4 Calcium oxalate (horizontal arrow) and cystine (vertical arrow) crystals. (Image courtesy of Jessie Hano, M.D.) (See Color Plate.)
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


