Fig. 6.1
Tissue triangulation gets lost when working away from the incision. As the distance between the incision and the operative field increases, the instruments begin to work parallel to each other and it becomes impossible to maintain tissue triangulation
Positioning and Assistants
Positioning of the patients during these cases is very important. As there is only minimal instrumentation through a single port, tissue retraction is limited. Because of this, gravity and native tissue attachments are frequently used as major tools of retraction. Therefore, it is many times necessary to put the patient in steep Trendelenberg position or airplane the patient to one side. It is beneficial to have an operating room table that can perform these maneuvers. In addition, placing a patient in yellow fin stirrups or in modified lithotomy position is also recommended as it allows the operating surgeon to stand in between the legs when accessing the upper abdomen. Owing to the use of extreme positions that may be necessary, the patient should be secured to the operating table using a bean bag or tape.
As in any abdominal case, good assistance is the key to the success of the procedure. In SILC, it is helpful to have a good assistant that has superior camera skills and is capable of operating a flexible and angled laparoscope if one is being used.
Access Devices, Ports, and Port Placement
There are many different access devices on the market today for single-incision laparoscopy. Early reports describe using a surgical glove or placing multiple traditional ports through the same fascial incision. Although economical, these are not durable and can result in a “swiss cheese” defect of the fascia. One study showed that the use of trocars without a single-incision device can result in loss of pneumoperitoneum and delay during the surgery [12]. It may be advantageous to use single-incision access devices which incorporate an expanding wound retractor that can maximize wound exposure. The use of a single-incision access device also increases the freedom of motion by distributing the anchoring points of the instruments over a two dimensional space (Fig. 6.2).
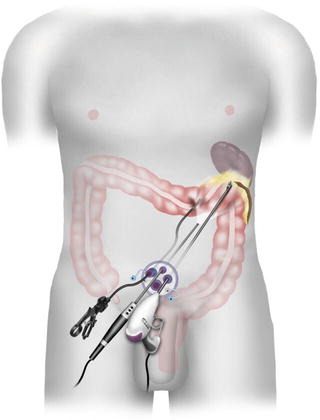
Fig. 6.2
The use of a single-incision access device increases the freedom of motion by distributing the anchoring points of the instruments over a 2D space
Location of Incision
For right colectomies, an incision can be made transumbilically or periumbilically. Both incision sites allow for the best visualization of the pathology and allow for the fascial incision to be extended without significant lengthening of the skin incision [10]. A transumbilical incision is beneficial because it allows for the best cosmesis, as the incision can be almost completely hidden within the umbilicus. For left-sided resections and rectal pathologies, either periumbilical or Pfannenstiel incision can be used (Fig. 6.3). The Pfannenstiel incision is preferred by the authors for left-sided resections because it provides some advantages over the periumbilical approach. The most technically demanding portions of the operation during a SIL left colectomy are splenic flexure take down and the distal rectal dissection and transection. In patients with a favorable body habitus, a Pfannenstiel incision allows distal rectal dissection and transection to be performed directly through the incision in hybrid open fashion. This site allows for good visualization of the region of concern and may decrease operative time.
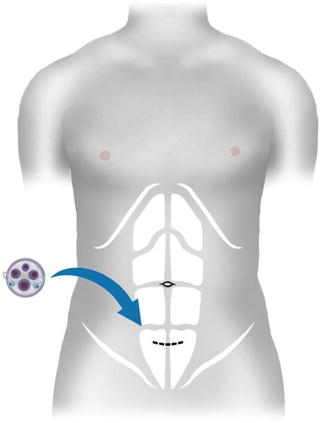
Fig. 6.3
For left-sided resections and rectal pathologies, a Pfannenstiel incision can be used
Once the access device is placed and exploration confirms the region of concern, specific placement of the ports within the access device can make the procedure easier. As with multiport laparoscopy, triangulation is tantamount. Although this can be difficult in single-port surgery, it is possible to recreate triangulation, albeit in a limited manner. We have found that if the apex of the triangle points toward the pathology, this can make the procedure less complicated.
Laparoscopes and Instruments
As with access devices and ports, there are no standardized laparoscopes or instruments for SILC. In a paper analyzing nine articles with seven different laparoscopic surgery teams, a variety of laparoscope sizes, tips, and angulations were used. No team used the same laparoscope [13]. The authors have found that a conventional angled (30 or 45°) laparoscope or a flexible tip scope is the best for these procedures. Straight laparoscopes are easy to use and most surgeons are familiar with them from multiport laparoscopic surgery. Flexible tip laparoscopes are more challenging to use and for this reason it is beneficial to have a camera operator who is accustomed to using this equipment. Flexible scopes allow the camera operator to stand away from the surgeon and can help avoid instrument and camera clashing. On the other hand, most flexible tip laparoscopes have a fairly long deflection tip which can make obtaining a wide overview of the operative field difficult. The incorporated end-on light source allows for avoidance of competition for space at the port site [14]. Longer scopes are also available and these can similarly be useful for positioning of surgeon and assistant. In addition, a smaller 5 mm scope can allow placement of a 10 or 12 mm instrument.
Although there are many flexible instruments available on the market, in our experience standard straight laparoscopic instruments are preferred. This has been recommended by other groups as well [5, 15]. Use of flexible instruments can be confusing and make the procedure more complicated because of counter-intuitive movements. Use of straight bariatric length instruments can be useful especially through Pfannenstiel incisions as they can also help to avoid crowding at the port site and have the added length to reach places such as the splenic flexure [15]. In addition, using instruments with variable lengths can allow manipulation of instruments externally in different planes, making it more likely to avoid collisions [16]. As experience broadens, use of curved and articulating flexible instruments may be incorporated.
Technique
As mentioned, many of the challenges with SILC are related to limited working space, visualization, and triangulation of instruments. As previously described, one way to avoid clashing of instruments externally is to use instruments of differing lengths. Some surgeons find it useful to use a combination of regular and bariatric length instruments and an extra-length laparoscope with a special adaptor which get the light cords out the way. Fixed curved shaft instruments that are specially designed for single-incision surgeries may also be useful. These instruments are reusable and have handles similar to straight instruments. The purpose of the curved tip is to restore some degree of the loss of triangulation (Fig. 6.4).

 Single Incision Laparoscopic Right Colectomy
Single Incision Laparoscopic Right Colectomy
 Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
 Robotic Single Port Colorectal Surgery
Robotic Single Port Colorectal Surgery
 Single Incision Laparoscopic Left Colectomy
Single Incision Laparoscopic Left Colectomy
 Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
 Hybrid NOTES Colectomy for Left-Sided Colonic Tumors
Hybrid NOTES Colectomy for Left-Sided Colonic Tumors




Related posts:
Single Incision Laparoscopic Right Colectomy
Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
Robotic Single Port Colorectal Surgery
Single Incision Laparoscopic Left Colectomy
Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
Hybrid NOTES Colectomy for Left-Sided Colonic Tumors
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
