The treatment of esophageal cancer has evolved considerably in the past decade and depends largely on the extent of disease at the time of presentation. For disease confined to the esophageal mucosa, endoscopic therapy is replacing esophagectomy as the standard of care. For locoregional disease, neoadjuvant chemoradiation followed by esophagectomy is the best strategy for optimizing long-term survival. In the minority of patents who present with metastatic disease, the prognosis is poor. Palliative therapies available for these patients include chemotherapy, radiation, endoscopic therapies to ameliorate obstruction or bleeding, and surgical intervention to optimize nutritional status or to relieve obstruction.
Key points
- •
Esophageal cancer encompasses adenocarcinoma of the tubular esophageal and gastroesophageal junction (cardia) as well as squamous cell carcinoma, two histologically and pathophysiologically distinct diseases.
- •
Biomarkers to aid in diagnosis, identifying at risk individuals, predicting response to therapy, and predicting overall prognosis are under development.
- •
Disease confined to the mucosa, without invasion of the muscularis mucosa, is amenable to endoscopic therapy, with a high cure rate.
- •
Patients with locoregional disease should receive multimodal neoadjuvant therapy before esophagectomy.
- •
Preoperative assessment should be performed, including cardiac and pulmonary evaluation as well as nutritional optimization and counseling.
- •
Curative esophagectomy can be performed with a variety of surgical approaches. Prognostic perioperative factors include complete R0 resection, the extent of lymphadenectomy, lack of blood transfusion, and absence of perioperative complications.
- •
Overall prognosis for patients with resectable locoregional disease depends on the pathologic depth of tumor invasion, degree of histologic differentiation, involvement of lymph nodes, and presence of distant metastasis. Five-year survival for surgery alone ranges from greater than 60% for stage 1B disease to ∼15% for stage 3C disease.
- •
Overall 5-year survival for patients with resectable locoregional disease receiving neoadjuvant chemoradiation and esophagectomy is ∼47%.
Introduction
Esophageal cancer is currently the sixth leading cause of cancer death worldwide. In the last 40 years, the incidence of adenocarcinoma has increased by 600%. The incidence increases steadily with age, with a median age at presentation of 68 years. Esophageal cancer encompasses 2 distinct histologic diseases: esophageal squamous cell cancer (ESCC), which predominates in China, India, and central Asia, and esophageal adenocarcinoma (EAC), which predominates in Western countries. Most esophageal tumors become symptomatic, usually heralded by dysphagia at late-stage disease. Understanding of the disease and its risk factors has improved in the last few decades but, despite significant advances in the oncologic and surgical care of these patients, overall survival is often poor.
Introduction
Esophageal cancer is currently the sixth leading cause of cancer death worldwide. In the last 40 years, the incidence of adenocarcinoma has increased by 600%. The incidence increases steadily with age, with a median age at presentation of 68 years. Esophageal cancer encompasses 2 distinct histologic diseases: esophageal squamous cell cancer (ESCC), which predominates in China, India, and central Asia, and esophageal adenocarcinoma (EAC), which predominates in Western countries. Most esophageal tumors become symptomatic, usually heralded by dysphagia at late-stage disease. Understanding of the disease and its risk factors has improved in the last few decades but, despite significant advances in the oncologic and surgical care of these patients, overall survival is often poor.
Biomarkers
There is ample investigation into the identification and clinical development of diagnostic markers that indicate the presence of cancer, markers of progression predicting an increased risk of developing cancer, markers that indicate a response to or provide an avenue for chemotherapy and biological therapy, and prognostic markers that correlate with overall survival. A 4-gene signature has been shown to predict survival in an independent validation cohort of patients with EAC. Those with none of the 4 gene markers had a 5-year survival of 58%; with 1 or 2 of the gene markers-year survival was 26%; and with 3 or 4 of the gene markers it was 14%. In a multivariate model adjusted for tumor-node-metastasis tumor staging, the 4-gene signature remained an independent predictor of mortality.
As the number and variety of targeted chemotherapeutics increase, there is interest in assessing oncologic pathway susceptibility to treatment. Multiple trials of targeted therapies including Herceptin, gefitinib, and erlotinib are ongoing. Her2 is present in approximately 15% to 20% of patients with esophageal adenocarcinoma and in the presence of metastatic disease should now be routinely assessed. Limited data suggest a survival benefit of Herceptin therapy in patients with advanced adenocarcinoma who are Her2 positive.
Treatment
Mucosal Disease
As the accuracy of noninvasive determination of tumor depth and the sensitivity for detection of local lymph nodes has improved, pretreatment staging has allowed resection of mucosal cancers without removal of the esophagus. The threshold for consideration of endoscopic treatment is currently at the muscularis mucosa, above which lesions are classified as T1a and below which lesions are classified as T1b and there is submucosal involvement. Invasion into the submucosa substantially increases the likelihood of occult lymphovascular involvement, documented to be 15% to 25% in reports of en bloc surgical resections. Endoscopic mucosal resection is currently an excellent treatment option for mucosal cancers and is used increasingly with and without ablative techniques.
Locoregional Disease
Neoadjuvant chemotherapy with radiation
Cisplatin-based chemotherapy in conjunction with radiation therapy has been shown to significantly improve survival compared with radiation therapy alone. The Radiation Therapy Oncology Group’s randomized trial of 4 cycles of cisplatin and 5-fluorouracil (5-FU) with 50 Gy of external beam radiation versus 64 Gy of radiation alone was closed prematurely because of a median survival of 14 months in the chemoradiation group versus 9 months in the radiation alone group and 5-year survival of 27% versus 0%. Approximately 85% of the study group had squamous cell cancer (SCC). Further, high-dose radiation does not seem to improve the outcomes of combined chemoradiation: the American InterGroup study showed no benefit of 64.8 Gy versus 50.4 Gy in conjunction with chemotherapy.
Multimodal neoadjuvant therapy before surgical resection has emerged as the optimal treatment of locoregional stage IIB to III cancers. Its role in submucosal clinically node-negative tumors remains to be defined, although a well-documented 15% to 25% prevalence of node metastases in the presence of submucosal lesions provides a rationale for its consideration. Several recent studies have shown survival benefits from preoperative neoadjuvant treatment. The Medical Research Council of the United Kingdom multicenter randomized control study of 2 cycles of cisplatin/5-FU separated by 3 weeks followed by surgery versus surgery alone showed an increase in median survival from 13.3 months to 16.8 months and 2-year survival from 34% to 43%. The Fédération Nationale des Centres de Lutte contre le Cancer (FNCLCC) and the Fédération Francophone de Cancérologie Digestive (FFCD) multicenter Phase III trial found similar results with disease-free survival improved from 21% to 34% and overall survival improved from 24% to 38%. The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial went on to show that preoperative and postoperative chemotherapy with epirubicin, cisplatin, and 5-FU was associated with improved survival versus surgery alone (3% vs 23%). Pennathur and colleagues studied neoadjuvant chemotherapy with cisplatin, 5-FU, and paclitaxel, and found that patients who were downstaged as a result of treatment response showed significant survival benefit.
Studies of preoperative chemoradiation have mostly been underpowered, but have trended toward showing a survival advantage versus surgery alone. The most recent and best of these trials, known as the Chemoradiotherapy for Esophageal Cancer followed by Surgery Study (CROSS), studied 366 patients with esophageal or junctional cancers. The study randomized patients to surgery alone or preoperative treatment with carboplatin and paclitaxel for 5 weeks in conjunction with 41.4-Gy radiotherapy. Pathologic compete response (pCR) occurred in 29% of the chemoradiation group, with improvement in median survival from 24 to 49 months, and 5-year survival from 34% to 47%.
Two recent studies have evaluated the value of chemoradiation compared with chemotherapy alone. A phase III trial comparing cisplatin, 5-FU, and leucovorin with or without 30-Gy induction radiotherapy for 126 patients with EAC showed that rates of pCR increased from 2% to 15%, rates of pN0 resection improved from 36% to 64%, and median survival improved from 21 to 33 months. A phase II trial of cisplatin and 5-FU with or without 35-Gy induction therapy for 75 patients with EAC showed that rates of pCR improved from 8% to 31% and median survival improved from 36% to 45%. Both studies were underpowered to show a significant survival advantage, but they suggested the usefulness of multimodal induction therapy.
It has been recognized that 10% to 15% of esophageal adenocarcinomas express HER2, and, to a lesser extent, other potentially targetable markers including epidermal growth factor receptor. Numerous trials are underway to evaluate the use of targeted biological therapies including cetuximab, trastuzumab, erlotinib, and gefitinib in conjunction with chemoradiotherapy.
Preoperative assessment and counseling
Esophagectomy is a potentially morbid procedure. Although it provides the best locoregional control and potential for cure, the risks of surgery are weighed against its benefit compared with alternate therapies. To ensure the selection of patients who would benefit most from esophagectomy, every effort must be made to assess the preoperative physiologic status of the patient. Several instruments have been developed for predicting perioperative mortality, identifying risk factors including age, preoperative weight loss; pulmonary, vascular, or cardiac disease; and both hospital and surgeon volume of esophageal resection.
In all patients, preoperative risk factor modification should include smoking cessation, blood pressure and blood sugar control, perioperative β-blockade if indicated, and optimization of nutritional status. Perhaps the most important modifiable risk factor, nutritional status can be difficult to augment for patients with esophageal disorders. Preoperative dilation, stenting, or feeding tube placement may facilitate caloric intake. The value of immunonutrition before surgery in reducing the risk of perioperative infections has been suggested and is currently under investigation.
Evaluation of cardiac (stress echocardiogram) and pulmonary function tests (PFTs) is necessary to identify the occasional patient with severe organ dysfunction. Preoperative nutrition counseling can be useful in easing the transition to the postsurgical period. Following esophagectomy, most patients experience a 1-month to 2-month adaptation toward full caloric intake. Patient education and participation are essential to optimizing long-term outcomes and quality of life.
Surgical approach
There are a variety of surgical approaches to esophageal resection, each with specific advantages and disadvantages. Factors important in selecting the optimal approach include the location of the tumor, extent of lymph node dissection, body habitus, prior chemoradiation therapy, comorbidities, and surgeon experience.
Ivor Lewis esophagectomy
Used for tumors of the midesophagus, distal esophagus, or gastroesophageal junction (GEJ), the Ivor Lewis esophagectomy involves a laparotomy and right thoracotomy, with intrathoracic esophagogastric anastomosis. The procedure begins with an upper midline laparotomy to examine for metastatic disease and confirm resectability. The triangular ligament is divided, the left lateral segment of the liver retracted medially, the gastrohepatic ligament divided, and the dissection carried down to the right crus. The phrenoesophageal membrane is divided along the right crus and over the esophagus, and then circumferential dissection of the esophagus is performed at the hiatus. The gastrocolic omentum is opened along the greater curvature of the stomach leaving a safe margin for the gastroepiploic artery and vein. The stomach is reflected anteromedially and the short and posterior gastric vessels are divided. The left gastric artery and vein are divided and all lymphatic tissue is swept with the esophagogastric specimen. The right gastric artery is carefully preserved as a component of the blood supply for the gastric conduit. A pyloromyotomy or pyloroplasty is performed to augment gastric emptying and the stomach is divided vertically with serial firings of a GIA stapler, maintaining a margin of 4 to 5 cm from the tumor. The stomach is commonly tethered to the esophagogastric specimen with sutures and the hiatus is enlarged to allow passage of conduit into the mediastinum. The distal esophagus is dissected slightly through the hiatus and the abdomen closed. The patient is then repositioned into the left lateral decubitus position for a right posterolateral thoracotomy.
For the thoracic portion of the procedure, the right lung is isolated and retracted, the thoracic esophagus mobilized, and the azygous vein divided. The esophageal dissection can be done either with or without a specific en bloc dissection of mediastinal lymph nodes. Periesophageal, subcarinal, and available paratracheal lymph nodes are dissected with the esophagus. Many surgeons prefer to specifically ligate the thoracic duct as it enters the thorax to minimize the potential for chyle leak. The esophagogastric specimen and conduit are delivered into the chest without torsion and the proximal esophagus is transected above the level of the azygous vein. An end-to-side esophagogastric anastomosis is then performed in the upper chest and the thoracotomy is closed.
A 3-incision esophagectomy
A 3-incision esophagectomy is similar to an Ivor Lewis procedure except that it usually begins with the thoracotomy portion of the procedure and the chest incision is closed without anastomosis to allow gastric pull-up to the neck for reconstruction. It is preferred in patients with tumors above the carina in which a transhiatal dissection may prove difficult or dangerous and in which a shorter esophageal remnant is necessary to provide adequate margins. The addition of a left-sided cervical esophagogastric anastomosis allows for wider resection margins for tumors of the upper and middle thirds of the esophagus. Rather than beginning in the abdomen, it is common to start in left lateral decubitus position with a right posterolateral thoracotomy. The esophagus is first mobilized from the thoracic inlet to the diaphragm, allowing definitive assessment of intrathoracic resectability before the abdominal portion of the operation. After the chest is closed, the patient is placed in the supine position and the abdominal portion is performed as described earlier for the Ivor Lewis esophagectomy.
A left cervical incision along the anterior border of the sternocleidomastoid muscle is created and the dissection is carried posteriorly with careful attention to the recurrent laryngeal nerve. The esophagus is divided and the specimen removed via the laparotomy incision. The gastric conduit is then pulled through the posterior mediastinum and an end-to-side or end-to-end cervical anastomosis performed. From the abdomen, the conduit is gently retracted to avoid redundancy and tacked to the diaphragm at the hiatus to prevent herniation.
En Bloc esophagectomy
En Bloc esophagectomy can be performed with either a cervical or intrathoracic anastomosis and requires a right thoracotomy. The procedure entails a specific effort to widely dissect all mediastinal and upper abdominal tissue from the carina to the celiac axis. The thoracic dissection plane begins outside the azygous venous system and includes resection of the thoracic duct and left pleura.
Transhiatal esophagectomy
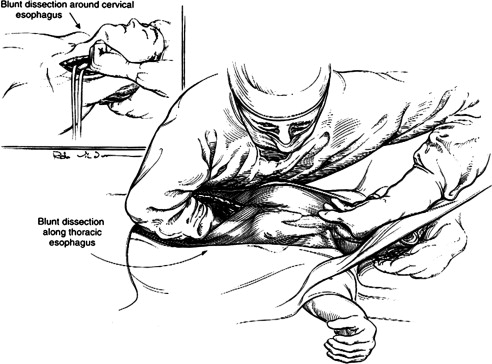
Transhiatal esophagectomy relies on dissection of the thoracic esophagus primarily through the abdominal incision ( Fig. 1 ). The distal third of the esophagus can usually be dissected under direct vision, whereas the proximal two-thirds are mobilized bluntly via the surgeon’s hand through the esophageal hiatus. The patient is placed in the supine position with the neck extended to the right, and the operation begins in a similar fashion to the procedure, with upper midline incision, exploration of the abdomen, exposure of the hiatus, mobilization of the stomach with preservation of the gastroepiploic arcade, mobilization of the esophagus to the hiatus, and ligation of the left gastric artery. A modified pyloroplasty is performed approximately and the diaphragm is incised anteriorly to widen the hiatus. The blunt dissection is first performed posteriorly along the aorta and spine, then anteriorly below the pericardium and trachea. Anterior and posterior dissection is usually straightforward. The lateral aspects of the esophagus including small vessels and the branches of the vagus nerves to the tracheobronchial tree is more difficult but can be accomplished with careful finger and hand dissection. An incision is made along the anterior border of the left sternocleidomastoid muscle, the platysma is divided, and the internal jugular vein and carotid sheath retracted laterally. Dissection of the cervical esophagus down the prevertebral fascia is performed. Blunt finger dissection is performed posteriorly and the tracheoesophageal groove is developed with concern for the recurrent laryngeal nerve. Mediastinal mobilization is then performed by blunt dissection with one hand entering the mediastinum via the cervical incision and the other via the abdominal incision and through the hiatus. This blunt dissection is continued with consideration for the posterior membranous trachea and the azygous vein until the operator’s fingers meet and circumferential mobilization of the esophagus is achieved. The esophagus is divided cervically, delivered into the abdomen, the stomach divided, and the specimen is removed. The gastric conduit is then prepared in the usual manner, pulled up through the mediastinum into the chest, and a cervical anastomosis is performed near the thoracic inlet. The gastric conduit is gently retracted to avoid redundancy and the hiatus repaired.