Introduction
Wilms’ tumor or nephroblastoma, is the most common renal tumor in children, accounting for approximately 7.6 cases per million children under age 15 [1]. Overall, about 6% of all childhood cancers arise from the kidney, and about 95% of these cancers are nephroblastomas. These are embryonal tumors that develop from immature kidney remnants. Wilms’ tumor (WT) was once thought to occur as a result of the classic single-gene, two-hit model described in retinoblastoma [2]; now at least 10 different genes have been shown to be involved [3].
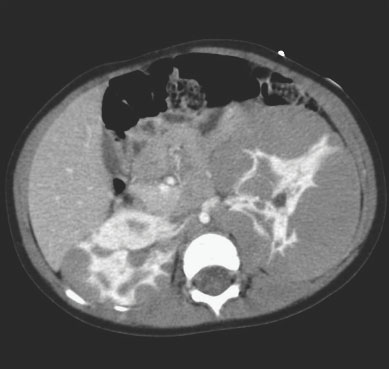
The highest incidence is in the first four years of life, although children of any age and adults also may be affected. The median age at presentation is between 3 and 4 years of age [1]. While solitary, unilateral lesions are most common, bilateral tumors occur in 7% of patients (Figure 40.1). Approximately 12% of patients have multiple lesions within one kidney [5]. The incidence is nearly equal between boys and girls worldwide, but in the United States, frequency is slightly higher in girls [4]. Based on the data from the Surveillance, Epidemiology, and End Results (SEER) program, prognosis is excellent, with an overall 5-year survival of over 88% for cases diagnosed between 1996 and 2004 [1]. Significant progress has been made in the treatment of WT mainly as a result of large collaborative groups, such as the Children’s Oncology Group (COG) and the International Society of Pediatric Oncology (SIOP), which have helped develop a multidisciplinary approach to therapy. Newer research emphasizes reducing morbidity of treatment for low-risk patients and improving efficacy of treatment for the subset of high-risk patients with poor survival.
Children with WT may present in many ways. Most commonly, an asymptomatic abdominal mass is found; however, other signs and symptoms at presentation include abdominal pain, gross hematuria, fever or acute abdomen due to tumor rupture. In less than 10% of patients, symptoms related to compression of adjacent structures may occur. These include varicocele, hepatomegaly, ascites, and congestive heart failure, resulting from extension into the inferior vena cava (IVC) or renal vein.
Wilms’ tumor generally has a great deal of histological diversity. The classic triphasic pattern, which mimics the cell types in the developing kidney, is composed of varying amounts of three cell types: blastemal, epithelial, and stromal. Each of these components responds differently to therapy and may influence outcomes [6]. Tumors with unfavorable histologic features, or anaplasia, are associated with increased relapse and death rates [7].
Clinical question 40.1
Should patients with hemihypertrophy or Beckwith–Wiedemann syndrome undergo screening for Wilms’ tumor?
Background
Wilms’ tumor has been associated with many identifiable syndromes, divisible into those characterized by overgrowth and those not associated with overgrowth. Hemihypertrophy or overgrowth of a body segment can occur as part of the Beckwith–Wiedemann syndrome (BWS) or an isolated problem, termed isolated hemihypertrophy. The BWS is a rare disorder of developmental anomalies characterized by excessive growth at the organ or cellular levels, with features such as macroglossia, nephromegaly, and hepatomegaly, as well as hemihypertrophy. It is caused by dysregulation of genes at chromosome 11p15, which control prenatal and childhood growth. The WT 2 gene (WT2) has also been identified on this site. Other rare overgrowth syndromes such as Simpson–Golabi–Behmel syndrome and Perlman syndrome have also been reported to be associated with WT.
The incidence of tumors in this population is 10–20%, including WT, adrenocortical tumors, and hepatoblastoma. The risk of tumor declines with age and by age 10 approaches that of the general population. Patients with hemihypertrophy and BWS have a risk of developing WT of the order of 4–10%, with about 21% of those patients presenting with bilateral disease.7 New evidence suggests that the risk of tumor development in BWS depends on the specific molecular mutation that causes BWS [8]. A prospective study of 168 patients with isolated hemihypertrophy demonstrated a 3% risk of WT [7]. Data from the National Wilms’ Tumor Study Group indicate that the 90% of WT are diagnosed by age 7, and 99% are diagnosed by age 10 [9].
Literature search
An extensive search was performed on PubMed for relevant articles using the following terms: “hemihypertrophy,” “Beckwith–Wiedemann syndrome,” “Wilms’ tumor,” “nephroblastoma,” “screening,” and “surveillance.” The references listed in identified publications were also reviewed. Three relevant studies were identified.
The evidence
A retrospective case series by Choyke and colleagues screened children with BWS or isolated hemihypertrophy and compared them to an unscreened group of patients [12]; 12 cases of WT were identified by screening and 59 cases were diagnosed in the unscreened population. None of the screened cases were late-stage WT, compared to 42% (25 cases) in the unscreened group. Three children in this series had a false-positive ultrasound and underwent invasive surgery for benign disease [10].
Another study from the UK by Craft et al. is a retrospective review of 41 patients with WT and BWS, isolated hemihypertrophy or aniridia [11]. This study did not show any difference in stage or outcome between patients who underwent tumor surveillance and those who did not.
Only one prospective, multicenter study, performed by Choyke and colleagues, has attempted to address the issue of tumor surveillance in isolated hemihypertrophy [12]. Of the 168 children in this study, 10 tumors developed, six of which were WT. Most study participants received an abdominal ultrasound every 6 months, but surveillance protocols varied amongst the study centers. One child developed a WT 5 months after the previous screening ultrasound, leading the authors to conclude that a screening interval of 6 months may be too long in these patients.
Comment
Based on the limited number of available studies, screening protocols appear to detect WT at earlier stages in children with BWS or isolated hemihypertrophy, potentially allowing these patients to undergo treatment with less morbidity. However, surveillance may lead to false-positive results, leading to unnecessary treatment, expense, and anxiety. Unfortunately, given the rarity of these overgrowth disorders and the low incidence of WT, a large, randomized controlled trial of surveillance is unlikely to occur.
Recommendations
Children with isolated hemihypertrophy should be screened with abdominal ultrasounds every 3–4 months until age 7. There is insufficient evidence to recommend screening beyond this age, given that 90% of WT are diagnosed by this age. Parents and families should be carefully counseled regarding the risk of tumor development and importance of adhering to surveillance protocols. Emerging evidence on epigenotyping of 11p15 in BWS and isolated hemihypertrophy patients may help delineate low-risk from high-risk individuals, but further clinical trials are needed in this area before screening recommendations can be amended.
Clinical question 40.2
What is the significance of certain chromosomal abnormalities, such as loss of heterozygosity of chromosomes 1p and 16q?
Background
The term loss of heterozygosity (LOH) refers to the inactivation of one allele of a gene in which the other allele has already lost its normal function. One of the most notable recent findings in WT is the significance of LOH at chromosomes 1p and 16q reported in the National Wilms’ Tumor Study Group (NWTSG) trials. Of the 232 patients enrolled in NWTS-3 and NWTS-4, LOH of chromosomes 1p or 16q was found in 11% and 17.2%, respectively. LOH of chromosome 16q was associated with a statistically significantly poorer 2-year relapse-free and overall survival, even when adjusted for tumor stage or histology. LOH of chromosome 1p was also associated with a lower overall and recurrence-free survival but the results were not statistically significant [13]. More extensive research has shed some light on this subject, allowing the use of LOH as a prognostic indicator in favorable histology WT (FHWT).
Literature search
A PubMed search was performed using the following terms: “loss of heterozygosity,” “1p,” “16q” and “Wilms’ tumor.” In addition we accessed the current COG protocol and reviewed the references listed.
The evidence
The NWTS-5 trial was designed to test the hypothesis that LOH of either chromosome 16q and/or 1p was associated with a worse prognosis in FHWT patients who were all treated with stage-specific treatment regimens. Of the 2021 WT patients enrolled in the study, 224 had LOH at chromosome 1p, and 360 had LOH at chromosome 16q. Patients with stage I or stage II FH tumors were at an increased risk of relapse or death with LOH at either one of the chromosomes. However, stage III/IV patients with LOH 1p alone did not have significantly worse outcomes than stage I/II patients when treated with stage-specific chemotherapy, suggesting that more aggressive chemotherapy may overcome the adverse effects of LOH.
Patients with LOH 16q alone had an almost identical overall survival as patients with no LOH (98.l% vs 98.4%, p = 0.60 in stage I/II and 92% vs 91.9%, p = 0.76 in stage III/IV). Most importantly, all FH patients with combined LOH (at both
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


