Fig. 27.1
High dorsal lithotomy position with surgeon and assistant sitting and viewing monitor in between the patient’s legs
Prone Jackknife
The surgeon and assistant stand on either side of the patient. Some surgeons favor this position for anterior lesions. One of the major drawbacks of the prone position is the difficulty managing the airway. This also means intubating the patient on the stretcher and then transferring the patient onto the operating room table, which translates into more operating room personnel and longer operating room setup time (see Fig. 27.2).

Fig. 27.2
Prone jackknife position with surgeon and assistant standing on either side of the patient
Port Setup and Instrumentation
Port Systems
Platforms approved by the Federal Drug Administration (FDA) for transanal access are the GelPOINT® Path port (Applied Medical, Rancho Santa Margarita, CA) and the SILS™ Port (Covidien, Mansfield, MA). Other access platforms that have been used are TriPort™ (Olympus, Wicklow, Ireland) system, Single-Site Laparoscopy (SSL) Access System (Ethicon Endo-Surgery, Cincinnati, OH), and the poor man’s glove port (see Figs. 27.3 and 27.4).
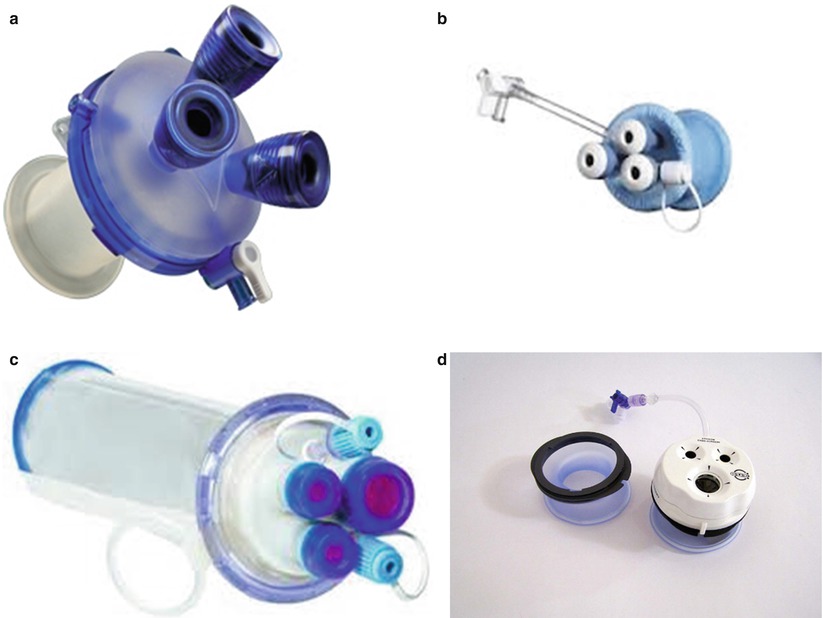
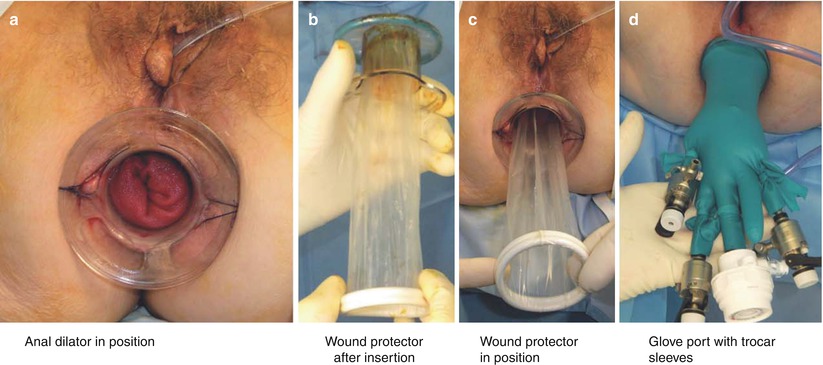
Fig. 27.3
Commercially available TAMIS platforms: SSL access system (a), SILS port (b), GelPOINT Path (c), TriPort (d)
Fig. 27.4
Glove port (a), anal dilator in position, (b) wound protector after insertion, (c) wound protector in position, (d) glove port with trocar sleeves
Three working ports are available in the GelPOINT® Path port, one for the camera and two as working ports. Any of the ports can be upsized to a 12 mm port if necessary. The advantage of this setup is that the surgeon has separation of the ports to allow for triangulation of the instruments. If necessary, a fourth port can be accommodated by piercing the gel cap directly.
Three working ports are also available in the SILS™ port. This port is particularly useful in patients with a narrow anal canal. The disadvantages of this platform are increased leakage of the pneumorectum and slippage of the port due to pliability of the used material. The access ports are positioned closer, which can make the triangulation more difficult.
The Olympus TriPort™ platform has three working ports. The top of the access platform can be exchanged to a 4-port version if an additional port is necessary. The length of the port is adjustable and can be tailored to the length of the patient’s anal canal offering a better fit and seal for the pneumorectum.
The Single-Site Laparoscopy (SSL) Access System accommodates two 5 mm instruments and one 15 mm instrument. The seal cap is designed such that the instruments can be directly inserted into the rectum without the need for trocars.
Several authors have successfully reported the poor man’s glove technique [17, 18]. A disposable circular anal retractor is secured to the skin, a wound retractor is then placed into the anal retractor, and a surgical glove is placed airtight over the wound retractor. Trocars are inserted through the fingertips of the glove. This port offers a less expensive alternative to all the above platforms. Additional manual support is necessary during each insertion and extraction of instruments, making it a floating platform.
Operating Instruments
A 5 mm camera with an angled tip allows a 360-degree view of the entire circumference of the rectal wall. One of the disadvantages of using standard laparoscopes is that the light cord interferes with the working instruments. Alternatively, a 5 mm flexible tip video laparoscope, EndoEYE™ (Olympus, Wicklow, Ireland) can be used; this is a low-profile system that prevents instrument collision outside as well as inside the rectal lumen (see Fig. 27.5). A standard laparoscopic CO2 insufflator is used to establish the pneumorectum with pressure set at 7–12 mm of Hg.

Fig. 27.5
Standard laparoscope and the Olympus EndoEYE
One of the working ports is used for a grasper and the other for an energy device. A 5 mm Maryland grasper is used as it provides a strong and precise grip of the specimen. The energy device can be an ultrasonic device and monopolar or bipolar cautery. Bipolar cautery and ultrasonic devices achieve excellent hemostasis but with added costs. Monopolar cautery can be used with a hook, spatula, scissors, or a needle tip, which can be bent. The advantage of using a monopolar cautery is that it can be used inside a 5 mm suction irrigator, which also aids in suctioning smoke. It also allows for a more precise plane of dissection.
Operative Steps (Table 27.1)
Table 27.1
Operative steps
Operative steps | Degree of technical difficulty (scale 1–10) |
|---|---|
1. Establishing access and pneumorectum | 2 |
2. Marking | 2 |
3. Dissection and excision | 5 |
4. Removal of specimen | 2 |
5. Closure | 7 |
Establishing Access and Pneumorectum
The anal canal should be well lubricated and dilated up to three fingers and the selected access platform should be inserted into the anal canal. The access platform should be then secured to the skin with a suture. Securing the port to the skin is an important step to provide an adequate seal for the pneumorectum and to prevent port slippage (see Video 27.1). The ports are inserted into the access channel. For the GelPOINT® Path port, the ports should be inserted into the Gel cap before securing the cap to the access channel. The handles of the instruments should be in horizontal position, away from each other to minimize instrument collision. Camera and instrument locations are dynamic throughout the procedure; they vary depending on the location of the lesion and area of dissection similar to laparoscopy. Pneumorectum is established using a standard laparoscopic CO2 insufflator up to a pressure of 7–12 mmHg. This pressure can be increased up to 20 mmHg to achieve adequate distention. At this point, the patient should be under general anesthesia, fully paralyzed without any spontaneous breathing to prevent any bellowing of the rectum. Smoke can be evacuated with short bursts of suction to avoid loss of pneumorectum.
Related posts:
 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Robotic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
 Transanal Endoscopic Surgery (TES)
Transanal Endoscopic Surgery (TES)
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach
 Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


