Fig. 11.1
A full set for laparoscopic surgery and a set for TEM
Modified TEM instrumentation
To perform “TETMR” the 12 cm rectoscope and the working insert of TEM instrumentation has been modified by Richard Wolf (Tuttlingen—Germany) according to the author’s suggestions.
1.
The shape of the 12 cm rectoscope has been modified by cutting the clarinet tip so two results have been achieved: a vertical section has been obtained and the rectoscope becomes significantly shorter (Fig. 11.2), therefore allows to work easily in the upper part of the operative field (Fig. 11.3). The modified distal edge of the rectoscope pressing the external anal margin makes possible to widen the canal anal and to perform a circular transversal incision of the mucosal layer between the anal verge and the pectinate line. The deep dissection is carried out in relation to the tumor extension as assessed by imaging (MR and Transanal US) performed before neoadjuvant treatment. The internal sphincter (that is easily identified), can be totally or partially removed if necessary.
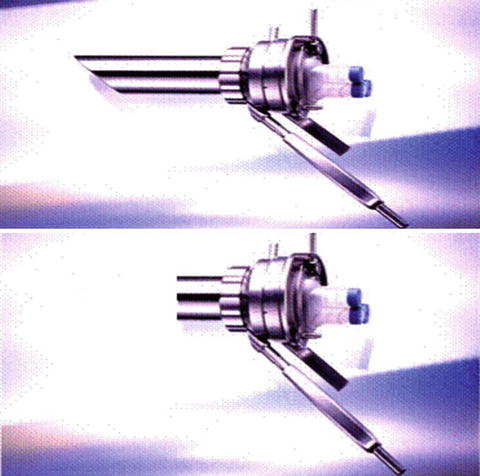
Fig. 11.2
A modified 12-cm rectoscope
Fig. 11.3
The upper part of the operative field
2.
The “working insert” (also named “operative faceplate”) has been modified so that the new model has a 10 mm hole to introduce a standard laparoscope locking it Fig. 11.4. Standard TEM optics have the advantages of a 3D view and an excellent magnification of the details due also to the perfect lighting; these technical features facilitate identification of the correct dissection plane, but at the same time have the default of a very narrow view of the operative field. This can cause the loss of the surgeon’s bearing. To avoid this situation it can be useful, once a large cavity has been created in the pelvis, to replace TEM optics with the 0° laparoscope that allows a wider view.

Fig. 11.4
The “working insert” (also named “operative faceplate”)
3.
Alternatively a 30°, 5 mm laparoscopy held by the assistant, can be placed in the sealing insert to increase lighting and to obtain a wider field of vision on the laparoscopic screen.
Patient’s Position
Posterolateral Lesions
The patient is placed on the operative table in Trendelenburg lithotomic position with the legs supported in stirrups.
Anterior Lesions
Patient is initially placed in prone position, for more detail see the chapter Tips and Tricks…page….
This position is generally employed only in case of anterior lesion in female patients. As matter of fact the dissection of the recto-vaginal septum is the most delicate part of the operation that requires to work in the best conditions. According to the TEM technique, the lesion must always be placed as close as possible to 6 o’clock of the operative field and patient must be rotated on the operating table to obtain the ideal operative placement during the whole surgical procedure. In male patient, the well-trained surgeon in TEM procedures can perform a 360° dissection maintaining the patient on the operative bed in the same position in order to minimize operative time.
Surgical Technique
Step 1 (by TEM Instrumentation)
A. Posterior Lesions
Surgery starts with a mucosal transverse circular incision at 1 cm from the lower margin of the neoplasia (A). The dissection may partially include the internal sphincter or it may follow the intersphincteric plane. A full-thickness incision is performed by electrocautery down to reach the “Holy plane” described by Heald. Then the surgeon continues the anterior isolation of the rectum rotating the operative bed both to the left and to the right in order to modify the working area until a 360° dissection has been achieved. The smooth dissection is facilitated by the CO2 insufflation that cranially pushing back the rectal stump. The excellent TEM view allows to preserve the integrity of mesorectal fascia (B–C) and parasympathetic pelvic plexus (D).
B. Anterior Lesions
Before starting the transanal access, in female patient it can be useful to stitch the uterus by laparoscopy technique to suspend it to the anterior abdominal wall. At the beginning of our experience the patient was placed in prone position then in the last three cases a supine position was utilized. Only in female patients with large tumors is the prone position is recommendable. The dissection starts by identifying the lower margin of the neoplasia and as for posterior lesions, it can partially enclose the internal sphincter or it may follow the intersphincteric plane. The next dissection is performed moving from the lateral side to the middle line, that allows to identify the recto-vaginal septum or prostatic capsule and seminal vesicles in males so completely removing the Denonvilliers’ fascia. By maintaining the prone position, the surgeon can continue the dissection rotating the patient laterally on both sides, so the complete mesorectum excision is reached. During the dissection a steel Trendelenburg position and the CO2 insufflation cranially push down rectal stump, obtaining a wide operative field. As soon as possible, to prevent further CO2 bowel insufflation, luminal liquid leak and tumor cell’s spillage, the distal cut edge of the rectal stump is closed with a purse string suture. Tumoral reimplantation is unlikely after radiotherapy.
Step 2 (by TEM Instrumentation)
If the patient was previously in a prone position, he must now be placed supine. By changing the working insert of TEM it is possible to work utilizing a 30°, 10 mm laparoscopic optic in order to obtain a wider view of the operative field (E). In this way the surgeon works utilizing the laparoscopic screen until the rectal stump with mesorectum is totally dissected as far as the peritoneal reflection is reached.
Step 3 (by TEM Instrumentation)
Dissection continues to the peritoneal reflection. This level can be easily identified by transillumination with an accessory laparoscopic optic. Then a washing of the residual cavity in order to sterilize the operative field is performed with Betadine©.
Step 4 (Laparoscopic Instrumentation)
Three (occasionally four) trocars are usually placed. The inferior mesenteric vein (IMV) is divided then the inferior mesenteric artery (IMA) beyond the origin of the left colic artery. The laparoscopic mobilization of splenic flexure and of the transverse colon is performed as usual.
Related posts:
 Single Incision Laparoscopic Right Colectomy
Single Incision Laparoscopic Right Colectomy
 Tricks and Routes to Success
Tricks and Routes to Success
 Robotic Single Port Colorectal Surgery
Robotic Single Port Colorectal Surgery
 Single Incision Laparoscopic Left Colectomy
Single Incision Laparoscopic Left Colectomy
 Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
 Hybrid NOTES Colectomy for Left-Sided Colonic Tumors
Hybrid NOTES Colectomy for Left-Sided Colonic Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


