Fig. 5.1
This graphic represents the correlation between less-invasive curative treatment of gastric cancer recurrence after partial gastrectomy and timing of follow-up
Table 5.1
Timing of follow-up: EGDS + biopsies (in anastomotic site and in the remnant mucosa)
Surgery | Follow-up |
|---|---|
Billroth-I/Billroth-II | |
(a) Benign | (a) Every 2 years 15–20 years after the initial surgery |
(b) Malignant | (b) Every 2 years 8–10 years after the initial surgery |
Total gastrectomy | |
(c) Benign | (c) No data |
(d) Malignant | (d) Every year 1–2 years after surgery |
Bariatric surgery | (e) On demand (clinical symptoms) |
5.1.2 Total Gastrectomy
After total gastrectomy , tumor recurrence can be subdivided as follows:
Distant tumor recurrence
Peritoneal tumor recurrence
Loco-regional tumor recurrence
Loco-regional tumor recurrence includes both endoscopically accessible tumor recurrence (at the anastomosis site or within loop) and endoscopically inaccessible tumor recurrence (lymph nodes or mass near the resected site) [16].
In the study of Lee et al. [17], among 215 patients with early gastric cancer submitted to total gastrectomy, there were no endoscopically accessible loco-regional tumor recurrences, while distant large masses were found in two patients at a 36-month follow-up. Among 622 advanced gastric cancer cases, 233 patients had tumor recurrence, in 24 of whom recurrence was endoscopically accessible. The endoscopic findings revealed stenosis in ten cases, mass in eight cases, ulcer in three cases, discoloration in two cases, and mucosal nodularity in one case.
Thus, distant tumor recurrence is more common than loco-regional tumor recurrence after total gastrectomy [16]. Endoscopic examination after total gastrectomy for gastric cancer has an important but limited role in the management of tumor recurrence.
5.1.3 Bariatric Surgery
The performance of bariatric surgery is escalating in order to treat the obesity epidemic, with multiple procedures that include:
Roux-en-Y gastric bypass (Fig. 5.2)
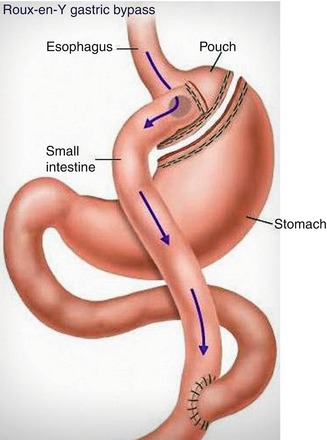
Fig. 5.2
This figure depicts the stomach’s appearance after Roux-en-Y gastric bypass
Vertical banded gastroplasty (Fig. 5.3)
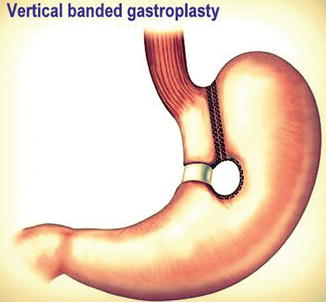
Fig. 5.3
Vertical banded gastroplasty is a purely restrictive procedure in which a small upper stomach pouch is created
Laparoscopic adjustable gastric banding (Fig. 5.4)
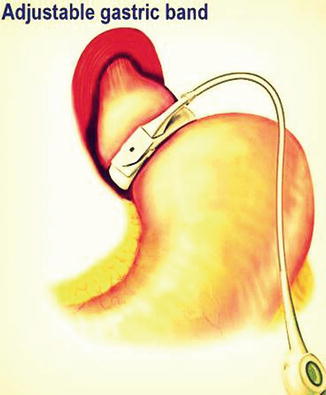
Fig. 5.4
Laparoscopic gastric banding is a purely restrictive procedure in which a prosthetic band is positioned around the entrance to the stomach
Sleeve gastrectomy (Fig. 5.5)
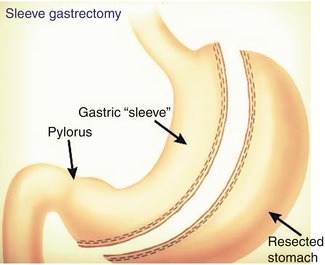
Fig. 5.5
With sleeve gastrectomy, a tubular stomach is created; after that, the majority of the greater curvature of the stomach is removed
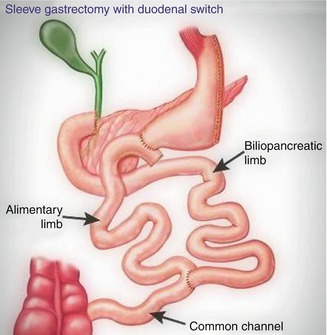
Sleeve gastrectomy with duodenal switch (Fig. 5.6)
Related posts:
 Impact of Flexible Endoscopy in the Evaluation of Digestive Anastomosis
Impact of Flexible Endoscopy in the Evaluation of Digestive Anastomosis
 Therapeutic Endoscopy for the Treatment of Benign Anastomotic Strictures
Therapeutic Endoscopy for the Treatment of Benign Anastomotic Strictures
 Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Small Bowel Surgery
Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Small Bowel Surgery
 Contribution of Endo-ultrasonography
Contribution of Endo-ultrasonography
 Augmented Endoscopy Imaging in the Study of Digestive Anastomosis: Does It Really Work and How?
Augmented Endoscopy Imaging in the Study of Digestive Anastomosis: Does It Really Work and How?
 Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Esophageal Surgery
Timing and Protocols of Endoscopic Follow-Up in Operated Patients After Esophageal Surgery

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


