Fig. 20.1
Large cystine stone (a) and coronal CT scan image (b) demonstrating a left staghorn calculus and a smaller left upper pole stone
Description
Access to the kidney is gained by using x-rays to direct a tube from the skin on your back to the kidney. The size of the tube placed can be up to 1 cm in width. Stones are extracted with a rigid telescope (Nephroscope or Renoscope; Fig. 20.2). Placed through the scope is a probe that has the dual advantage of using ultrasonic and pneumatic energy to fragment the stone (See Fig. 20.3). The ultrasound emitter at the end is typically used to drill holes and break the stone in to small pieces (Fig. 20.4). A pneumatic hammer, which acts like a jackhammer, can also be employed to break the stone (Fig. 20.5). After the stone is broken, one extracts the stones fragments through a tube. After the procedure is complete, the large 1 cm access tube is exchanged for a smaller drainage tube (typical 0.4 cm in width), called a nephrostomy tube.


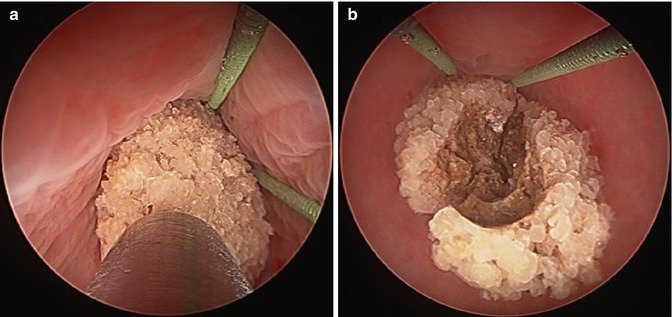
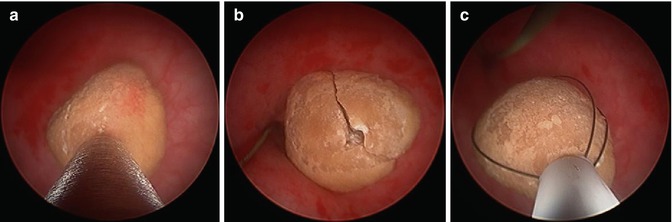
Fig. 20.2
Image of a nephroscope used to look inside the kidney
Fig. 20.3
Image of Lithoclast
Fig. 20.4
Nephroscopic view of the renal pelvis demonstrating large renal stone. Lithoclast using the ultrasonic lithotripter (a) and the resulting large stone cavity created (b)
Fig. 20.5
Lithoclast using the pneumatic lithotripter used to fragment stone (a); Stone cracked (b) and fragment removed (c)
Advantages
Able to remove very large stones, multiple small stones, even stones that encompass the entire kidney.
Disadvantages
Usually requires hospitalization. After the procedure, the nephrostomy tube coming out the patient’s back might need to remain for several days. This can be uncomfortable, especially when sleeping. With the nephrostomy tube in close proximity to the lungs, rarely patients can have air (pneumothorax) or fluid (hydrothorax) build between the lung and the chest wall. This may require further procedures to rectify.
Treatment
Ureteroscopy: Going to great lengths to treat your stone!
Indications
Smaller stones of the kidney. The widths of all the stones when summed together should be less than 1.5 cm.
Description
Technological improvements have allowed for the manufacture of very small telescopic instruments, called ureteroscopes (See Fig. 20.6). A Urologist will advance the scope through the urethra and bladder, up through the ureter and extending into the kidney. Once in the kidney, the stone is typically pulverized with a powerful laser to manageable-sized pieces. These pieces must be small (<0.3 cm) so that they can be extracted with a basket deployed through the ureteroscope (Fig. 20.7). Several passes are often required to remove the entire stone burden. A ureteral stent is placed after the procedure to allow the ureter to heal from the trauma of the ureteroscope. The stent is usually removed 1–3 weeks later in the office.

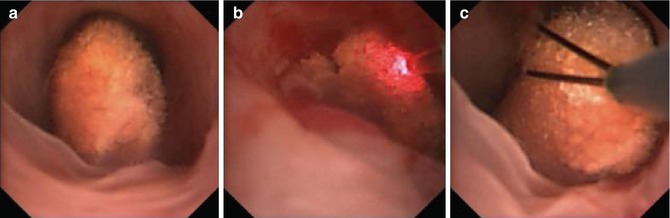
Fig. 20.6
Image of flexible ureteroscope
Fig. 20.7
Ureteroscopic view of stone within the renal pelvis (a); laser ablation of stone (b); stone in basket (c)
Advantages
This is a minimally invasive approach. There are no incisions as the approach is via the urethra. A good amount of stone can be treated. This is an ambulatory procedure, and most patients go home the same day of surgery.
Disadvantages
It is impractical for a large amount of stones.
Treatment
Extracorporeal Shockwave Therapy (ESWL): The Stone Breaker!
Indications
Stones up to 1.5 cm in the kidney
Description
ESWL is a very appealing way to treat kidney stones is by utilizing shockwaves generated outside the body. Technology is such that an ultrasound wave can be targeted so that its energy is focused on a target stone (Fig. 20.8). There are no incisions. A patient will be sedated for up to 3,000 shockwaves to be delivered. This procedure is usually <45 min and can be performed under ultrasound or fluoroscopy (x-ray) guidance to localize and monitor the stone. The stone fragments into small pieces, which the patient subsequently urinate out over the following several days and weeks.

Fig. 20.8
Dornier Compact Delta II lithotripter (Courtesy of Dornier MedTech)
Advantages
No incisions! No telescopes (ureteroscopes) in the body. Same-day surgery.
Disadvantages
This procedure does not work well for treating hard stones, like cystine, calcium oxalate monohydrate and calcium phosphate stones. The stone may not fragment into small enough pieces, which may necessitate a Urologist placing a stent and extracting the stones with a ureteroscope. This procedure is contraindicated in pregnancy. One retrospective study in the literature describes the increased risk of diabetes and hypertension following ESWL [1]. This report remains controversial, as other reports do not support these findings.
Stones in the Ureter
Urinary stones lodged in the ureter can often be painful! Remember that discomfort from stones is most often caused by the blockage of urine flow from the kidney to the bladder. Historically, these stones required open surgical extraction if they failed to pass. For a period of time, Urologist may have attempted to retrieve a stone by blindly placing a small basket in the ureter to snare it. This was associated with particular risk as it had a much higher rate of injuring the ureter compared to more modern techniques. With modern techniques described below, this major complication is exceedingly rare.
The use of ureteroscopy has really become the main stay for urologists to help a patient remove a ureteral stone that will not pass without surgical intervention.
Treatment
Open Surgical Stone Extraction
Indications
Simultaneous abdominal or pelvic surgery
Description
Once the standard of care many years ago, this invasive method of removing stones from the ureter is rarely indicated in the era of modern ureteroscopy. It treatment option is infrequently utilized today unless it is combined with another operation (e.g. open surgical removal of the uterus). Even in this scenario, the urologist may recommend to do a staged procedure in which the stone is removed ureteroscopically prior to the abdominal operation.
Advantages
When combined with another abdominal procedure, the stone extraction portion can be rather quick.
Disadvantages
This represents the most invasive means to remove a stone from the ureter (unless the patient is already undergoing a major abdominal incision for another reason). In spite of affording the urologist direct visualization of the stone, they may still have difficulty locating it.
Treatment
Ureteroscopy with Stone Extraction
Indications
Urinary stones of any size in the ureter that fail to pass spontaneously.
Description
Similar to stones in the kidney, ureteroscopes can be used to remove ureteral stones. Depending on the patient’s anatomy, either flexible and/or semi-rigid ureteroscopes will be used.
The scope is advanced through the urethra and into the bladder. From there, it is guided by a direct visualization with a camera into the appropriate ureter and to the level of the stone. Uncommonly, the Urologist may need to use a small balloon and dilate the ureter to accommodate the ureteroscope. More commonly, an open sheath, called an access sheath (Fig. 20.9), can be advanced into the ureter (i.e., a tube within a tube approach), which aids to protect the ureter before the ureteroscope is inserted.





