Fig. 9.1
Cystoscopic view demonstrating enlarged lateral lobes of the prostate
Surgical Factors
Summary Stone Facts
Not all weight surgical procedures are the same and the risk of stones can be quite different.
Patients with resection of their gastrointestinal tract have an increased risk for stones.
The portion of the intestinal tract resected will influence the type of stone the patient will form.
Gastric Bypass Versus Gastric Banding: Does Bariatric Surgery Increase Your Risk of Stones: Fact or Fiction?
Patients who undergo gastric bypass procedures develop changes in their urinary chemistry that increase their risk for developing nephrolithiasis. Patients who undergo the most common type of gastric bypass surgery, the Roux-en-Y (RYGB), whereby creation of a small gastric pouch so food bypasses part of the small intestines, are at increased risk for calcium oxalate kidney stones beginning 6 months after surgery. In one study, the risk of stones was 7.65 % compared to 4.63 % in the control group [12]. The added kidney stone risk is thought to be due to changes in the urinary chemistry. Patients who have undergone Roux-en-Y gastric bypass surgery have excess oxalate and low levels of citrate in their urine after the procedure.
Other types of weight loss surgery, including gastric banding, is not associated with an increased risk for kidney stones or kidney stone surgeries [13].
Recommendations to reduce an individual’s risk for stones following gastric bypass is to increase fluid intake, limit oxalate containing foods, reduce sodium intake and red meat consumption.
Small Bowel Resection
Short bowel syndrome, is a condition that generally occurs when portions of the small intestines are surgically removed. It causes an inability to properly absorb fat and nutrients. These patients may develop steatorrhea, a condition whereby there is excess fat in the stool. Calcium may bind to the unabsorbed fatty acids, resulting in a condition referred to as saponification. This allows increased concentration of free oxalate in the bowl lumen to be absorbed in the colon resulting in hyperoxaluria. As a result of low urine volume, Hypocitraturia, hypomagnesuria and hyperoxaluria, these patients are at an increased risk of developing calcium oxalate stones. Prevention of stones involves a low fat, low oxalate diet, increased fluid consumption to increase urine volume, oral calcium to bind oxalate in the gut lumen and citrate and magnesium replacement [14].
Ileostomy and Colon Resection
Patients with an ileostomy and individuals with a colon resection have a tendency to chronic volume contraction due to loss of water, bicarbonate and potassium in diarrheal stool, leading to reduced urine volumes. These individuals also have decreased absorption of citrate and magnesium, resulting in less inhibitory action on calcium oxalate crystallization. As a result, these patients have a tendency to produce calcium oxalate stones. These patients also form uric acid stones as a result of bicarbonate loss in the ileostomy resulting in acidic urine combined with watery stools and low urine volume. Therapy is directed by alkalization of the urine to a pH of 6.5, increasing urine volume to increase the solubility of uric acid to prevent crystallization [14]. These stones are often very difficult to prevent without decreases in diarrhea/ileostomy losses.
Medication Factors: Drug Induced Renal Calculi
Summary Stone Facts
Urinary tract stones can be produced by a number of medications used to treat a variety of medical conditions.
Some medication can treat one type of stone but produce a different stone type.
Medication may produce a metabolic abnormality or the drug itself may crystallize in the urine to produce a stone. Correcting this metabolic abnormality may prevent the stone from forming.
Other drugs may form stones by crystallizing in the urine. Preventing these stones usually involves discontinuation of the medication and initiation of an alternative therapy.
Nephrolithiasis may be produced by a number of prescription and nonprescription drugs used to treat a variety of medical conditions. These drugs may lead to metabolic abnormalities that initiate the formation of urinary tract stones. Approximately 1–2 % of renal calculi are drug-induced. Drugs that induce metabolic calculi include diuretics, carbonic anhydrase inhibitors, and abuse of laxatives. Correcting the underlying metabolic abnormality may reverse or eliminate the stone formation process.
Urinary calculi can also be produced by medications when the drugs crystallize (i.e., urinary supersaturation) and become the primary component of the stone. Medications that initiate this process include magnesium trisilicate, Ciprofloxacin, sulfa medications, triamterene, indinavir, and ephedrine with or without guaifenesin. When this situation occurs, cessation of the medication is usually necessary to reverse this process.
Loop Diuretics
Bumetanide and Furosemide
Bumetanide and Furoside are used to treat hypertension, edema and hypercalcemia. They inhibit both sodium and calcium resorption in the thick ascending limb of the loop of Henle. In addition to exerting a diuretic effect, this mechanism of action produces a hypercalciuric state, resulting is an increased risk of calcium oxalate stones. In low birth weight infants receiving furosemide therapy, stones have been identified in up to 64 % of infants. These stones are radiopaque on plain x-ray studies.
Carbonic Anhydrase Inhibitors
Carbonic anhydrase inhibitors, such as acetazolamide (Diamox), is used to treat patients with glaucoma, altitude sickness, congestive heart failure, seizure disorder, pseudotumor cerebri and urinary alkalinization. This medication acts in the proximal tubule where they block resorption of sodium bicarbonate. Extended use of carbonic anhydrase inhibitors may lead to a hyperchloremic metabolic acidosis, in which urinary pH is increased and urinary citrate is decreased. Consequently, long-term use of this drug can increase the risk for the production of calcium phosphate stones.
Laxatives
Laxatives are used primarily to treat constipation. Abuse of laxatives can result in diarrhea, nausea and vomiting. Significant water loss can result in low blood pressure, cardiac problems and kidney related issues, including stones. Patients with chronic diarrhea secondary to laxative abuse often have low urine volumes and acidic urine pH. Ammonium acid urate calculi (Fig. 9.2) are more frequent among patients with persistent diarrhea associated with laxative abuse.
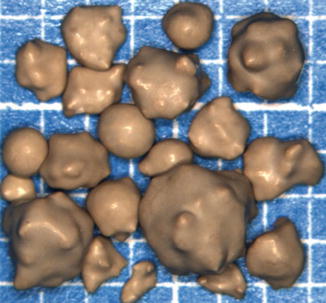
Fig. 9.2
Ammonium acid urate stone (Courtesy of Louis C. Herring & Co., Orlando, FL)
Ammonium acid urate calculi are radiolucent on plain X-rays unless mixed with calcium. Cessation of laxatives may lead to the correction of the urinary abnormalities. In addition, counseling by an internist, psychiatrist or psychologist and a registered dietician is recommended to treat the patient’s eating disorder.
Magnesium Trisilicate
Silica is a universally distributed element and frequently found in foods such as vegetables, whole grains, seafood and drinking water. Magnesium trisilicate is an antacid medication that is available without a prescription for the treatment of symptoms of gastroesophageal reflux disease. Although dietary silicate is readily excreted in the urine, the consumption of excessive amounts of magnesium trisilicate can produce silicate stone formation. Silicate calculi are poorly radiopaque and easily treated with conventional lithotripsy methods. Prevention of Stone recurrence can be prevented if the patient discontinues the use of magnesium trisilicate antacids.
Antibiotics
Ciprofloxacin
Ciprofloxacin is a fluoroquinolone antibiotic used to treat complicated and uncomplicated urinary tract infections. It is nearly insoluble at neutral or alkaline pH and crystallizes in excreted alkaline urine of animal models. In patients, ciprofloxacin crystalluria can form when dosages are greater than 1,000 mg and the urine pH is greater than 7.3. Ciprofloxacin calculi are radiolucent on plain radiography and are best identified with contrast imaging studies.
Sulfa Medications: Sulfonamides
The administration of sulfonamides can be complicated by the development of sulfa crystalline aggregates of these drugs in the urine; stones are radiolucent.
Sulfamethoxazole-Trimethoprim
Sulfamethoxazole-trimethoprim (Bactrim) is a commonly employed antibiotic to treat infections.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


