Fig. 3.1
We started the percutaneous renal surgery in supine position with the same protocol we have been using in prone position. Lithotomy position was used to catheterize the ureter, and then we changed the field placing the patient in the Valdivia position and leaving the transurethral way with the perfusion of contrast and dye through the catheter
3.3 Discovering the Endoscopic Combined IntraRenal Surgery (ECIRS)
A short time after starting to operate in the Valdivia position, we found ourselves, at the end of a PNL, with a large number of fragments dislodged in the distal ureter. This particular case was of a woman previously treated with ESWL for a stone of considerable size in the left kidney. After fighting a long time to remove the whole Steinstrasse, my assistant, Dr. Aurelio Jorge, asked for a rigid ureteroscope, dismantled the field, and improvised a transurethral access with the patient in supine position and the knees flexed (Fig. 3.2). We solved the case very quickly and numerous fragments pushed upwards were easily extracted through the Amplatz sheath.
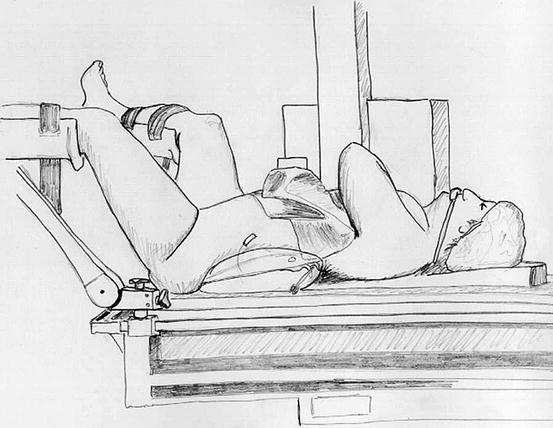
Fig. 3.2
The residual fragments and the Steinstrasse after an incorrect indication to ESWL forced us to perform transurethral URS and PNL. The lithotomic position was uncomfortable for performing both procedures simultaneously, and the stirrups could cause pain to the patient’s legs
This was, as far as I remember, the first “rendezvous,” opening the way to a new concept in endourology: the simultaneous transurethral and percutaneous access to the whole urinary tract.
3.4 In Search of the Best Position
Since then we began to place the patient in the lithotomic position, placing the ureteral catheter almost simultaneously to the percutaneous puncture. Perfusion through the catheter was no more necessary as the assistant could inject contrast when needed, and if we thought it convenient, we could also perform a transurethral URS.
Although, the classical lithotomic position was uncomfortable, and above all, depending on the type of leg support employed, it could produce pain to the lower limbs during the postoperative period, especially after long procedures. We gradually started changing the position of the ipsilateral leg, looking for more ergonomic leg holders until we found a position comfortable for both surgeon and patient (Fig. 3.3).
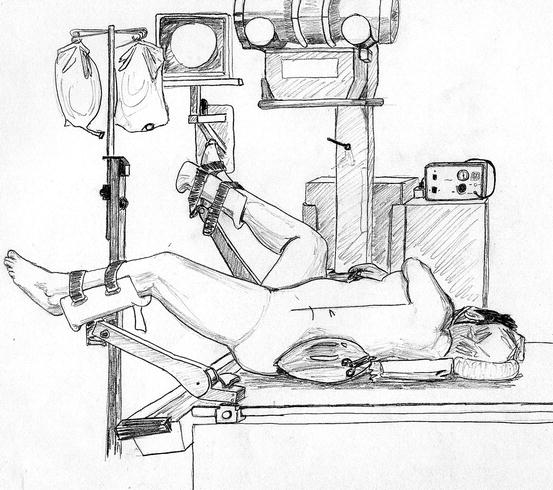
Fig. 3.3
Gradually we developed a more comfortable position for both patient and surgeon, finding more appropriate leg holders. The ipsilateral leg was extended with a small knee flexion, and the contralateral leg was well abducted
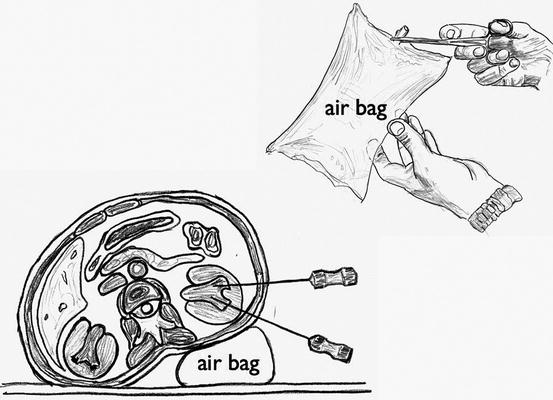
We always used a three-liter saline solution bag filled with air clamped with a Kocher forceps, allowing volume control until the best position was found (Fig. 3.4). The bag can be very full with the patient more sideways if we have to enter through a posterior calyx and can contain less air with the patient practically in supine position if we have a very accessible anterior calyx. We have tried to replace the irrigation bag by other devices, but by now we always came back to it.