CHAPTER 8 The contracted bladder
HISTORY AND EXAMINATION
Examination is usually unremarkable although there may be some supra-pubic tenderness.
MANAGEMENT
In most cases, treatment of the underlying cause will have already failed to halt disease progression and therefore operative treatment is indicated. Most cases of contracture are treated by cystectomy and urinary diversion or bladder reconstruction (see Chapter 5). More conservative treatments such as cysto-distension do not produce long term symptomatic relief.
Urodynamics in bladder contracture
Pressure/flow cystometry
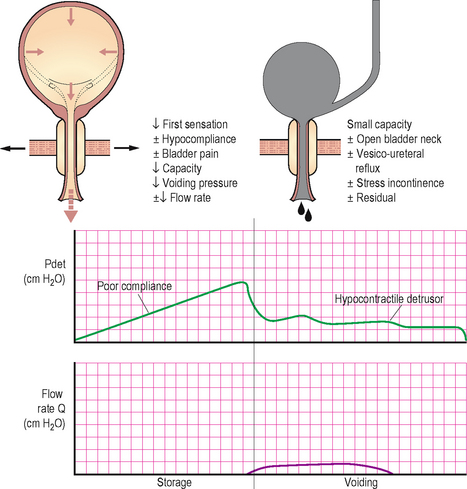
Bladder contracture is best assessed with video urodynamics. Often during the filling phase there is a reduction in the volumes at which bladder sensations such as the first sensation of filling occur and the maximum cystometric capacity (MCC) is also reduced, giving the urodynamic appearance of bladder hyper-sensitivity. The compliance of the bladder is also often severely reduced, due to fibrosis of the detrusor muscle (Chapter 4). The findings must be interpreted in the context of data from a bladder diary and an assessment of anatomical bladder capacity.
Voiding may also be affected; fibrosis of the detrusor will lead to inefficient contractions and detrusor underactivity (Chapter 6). The result will be a weak detrusor contraction coupled with a poor flow rate, prolonged voiding and raised PVR; often the patient uses abdominal straining to aid voiding (low pressure, low flow voiding).
Video screening will not only determine if incontinence or vesicoureteric reflux is present but usually shows that the bladder is small and unusually spherical in appearance (Figure 8.1).
< div class='tao-gold-member'>




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


