(1)
Gastroenterology and hepatology, Chinese PLA General Hospital, Beijing, China, People’s Republic
Abstract
In Chap. 5 aspects of techniques in tunnel establishment are discussed: (1) Patient positions including left lateral position, supine position and supine position with right should lifted; (2) The location where the submucosal tunnel is established should be in line with the location of the lesion to be resected and have an appropriate distance from the margin of the targeted lesion; (3) The types of entry incision during esophageal tunnel technique generally include the transverse incision and the longitudinal incision, while the arc incision is a third mutated type of incision from tunnel technique. The different types of incisions are used in different cases and have different techniques of their sealing; (4) The healing process was related to the corresponding management measures before and after operation, mainly the operation related factors, food intake, medication and individual differences; (5) How to keep a relative aseptic operation not only concerns operation safety, but has a great influence on the further development of the technique.
The entry incision of the tunnel is a window where the endoscopy enters the tunnel, and this directly influences the intra-tunnel pressure, the convenience of passing through the tunnel, and the degree of difficulty of postoperative sealing of the entry incision. Different types of entry incisions may be needed for best treat lesions of different locations. However, for lesions of the same location, the best incision type could be chosen based on the preference of the operators and on the localized anatomy.
4.1 Patient Positions
Left lateral position (Fig. 4.1a): left lateral position is the routine position for endoscopic examination. All physicians conducting endoscopic examinations should be well aware of the anatomic orientation of the esophageal wall under this position so as to choose the optimal esophageal wall for tunnel establishment in different operations [1–3].


Fig. 4.1
Patient positions for tunnel technique. (a) Left lateral position. (b) Supine position. (c) Supine position with right should lifted
Supine position (Fig. 4.1b): supine position is the routine position for the anesthetist to perform intubation, which is suitable for the operation of lesions located at certain parts of the esophageal wall. However, the head position of the patients make it slightly more difficult to push the endoscope forward [4, 5].
Supine position with right should lifted (Fig. 4.1c): this is a position between the left lateral position and the supine position, with less distorted neck and the mouth of the patient directed towards the operator.
4.2 Location and Orientation of Tunnel Establishment
The site where the submucosal tunnel is established should be in line with the site of the lesion to be resected. For a mucosal lesion, the upper entry incision site generally lies above the oral mark line, and the lower entry incision site lies below the anal mark line (Fig. 4.2a, b). For SMTs originating from muscularis propria, the entry incision should be done at the oral side of the tumor and about 2.5 cm above the tumor to establish a tunnel (Fig. 4.2c). For esophageal achalasia, although peroral endoscopic myotomy could be performed at any side wall of the lower esophagus and the cardia, it is best to choose a side wall farthest away from the descending aorta and the inferior vena cava to minimize the chance of hemorrhage, so the lesser curvature side wall of the cardia is recommended for tunnel establishment and myotomy because it has a smooth curvature during the establishment of the tunnel and will less possibly cause a tunnel perforation (Fig. 4.2d). For lesions outside of the muscular propria, the entry incision should be at the oral side of the lesion and about 3 cm above the lesion to establish a tunnel throughout the muscularis propria to the lesion outside the digestive lumen.
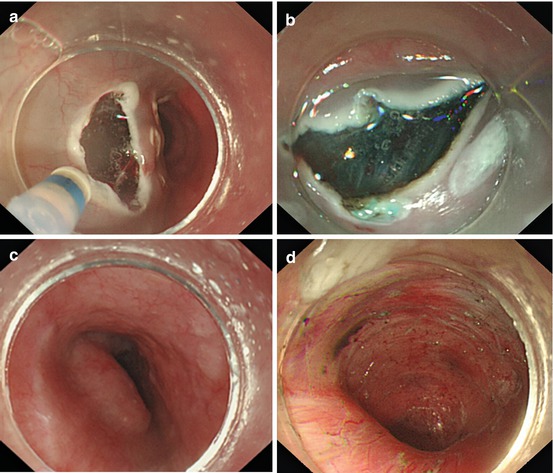
Fig. 4.2
Location of tunnel establishment. (a) For a mucosal lesion, the upper entry incision site lies above the oral mark line. (b) For a mucosal lesion, the lower entry incision site lies below the anal mark line. (c) For SMTs originating from muscularis propria, the entry incision at the oral side of the tumor and about 2.5 cm above the tumor. (d) For esophageal achalasia, tunnel is established in line with the lesser curvature of the cardia which is smooth and not vulnerable to tunnel perforation
The entry incision should be located at the anal side of the lesion during peranal establishment of a submucosal tunnel, which is contrary to the choice of the oral side of the lesion for entry incision during peroral tunnel establishment, but the other procedures of tunnel establishment are the same between the two operation routes.
4.3 Incision and Sealing of the Entry of the Tunnel
The types of entry incision during esophageal tunnel technique generally include the transverse incision and the longitudinal incision, while the arc incision is a third mutated type of incision from tunnel technique.
4.3.1 Longitudinal Incision
The longitudinal incision is firstly clinically reported by Inoue [6]. In this entry incision, a longitudinal incision of the esophageal mucosa deep into the submucosal layer is performed after submucosal injection, and the length of the incision is about 1.5–2 cm.
The procedure of performing the longitudinal incision: (1) Choose the site for incision (Fig. 4.3a); (2) Perform submucosal injection to lift the mucosa appropriately (Fig. 4.3b); (3) Use needle-knife or Dual knife to longitudinally incise the mucosa deep into the submucosa with a length of 1.5–2 cm (Fig. 4.3c); (4) Advance the endoscope into the submucosa to continue the submucosal injection in the distal end of the incision (Fig. 4.3d), and then dissect the submucosal tissue along the two sides of the incision, so that the transparent-cap attached endoscope could enter the submucosal layer smoothly.
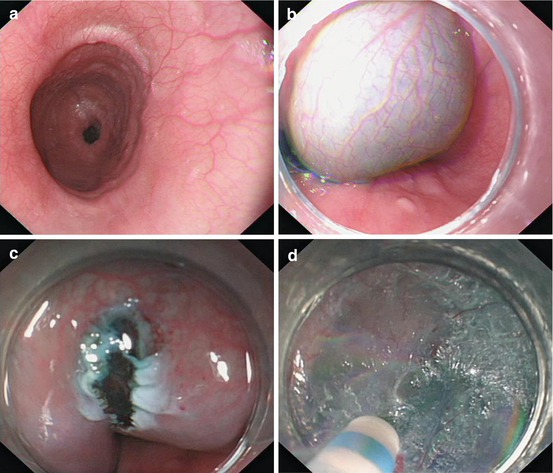
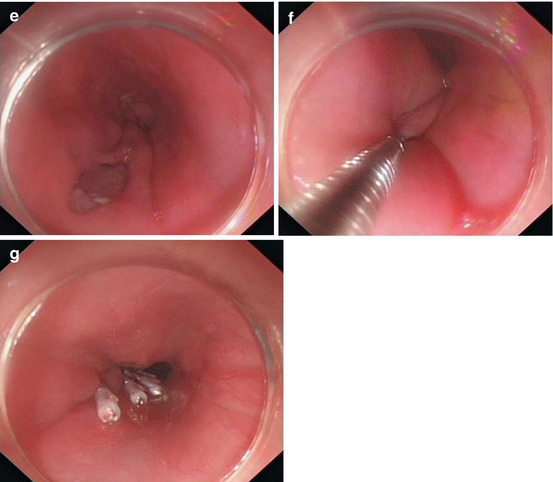
Fig. 4.3
(a) Choose the site for incision. (b) Submucosal injection to lift the mucosa. (c) Longitudinal incision. (d) Advance the endoscope into the submucosa. (e) Longitudinal incision after myotomy. (f) Release of the first hemostatic clip. (g) Completely sealed longitudinal incision
Sealing of the longitudinal incision (Fig. 4.3e–g): Seal the incision from the distal to the proximal end with hemostatic clips. The interval between each two adjacent clips should be about 2–3 mm and the clips should rich reach the depth of the lower mucosal tissue.
Indications of the longitudinal incision: lesions of or outside the muscularis propria.
4.3.2 Transverse Incision
The transverse incision is firstly clinically reported by Linghu et al. [1]. In this entry incision, a transverse incision of the esophageal mucosa deep into the submucosal layer is performed after submucosal injection, and the length of the incision is about 1.2–1.5 cm.
Related posts:
 Indications of Tunnel Technique
Indications of Tunnel Technique
 Principle of Digestive Endoscopic Tunnel Technique
Principle of Digestive Endoscopic Tunnel Technique
 Experimental Researches of Digestive Endoscopic Tunnel Technique
Experimental Researches of Digestive Endoscopic Tunnel Technique
 Tunnel Technique for SMTs Originating from Muscularis Propria
Tunnel Technique for SMTs Originating from Muscularis Propria
 Tunnel Technique for Digestive Mucosal Lesions
Tunnel Technique for Digestive Mucosal Lesions
 Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


