CHAPTER 1 SURGICAL AND RADIOLOGIC ANATOMY*
LIVER
GROSS ANATOMY
The liver lies under cover of the lower ribs, applied to the undersurface of the diaphragm, and is astride the inferior vena cava posteriorly. Most of the bulk of the liver lies to the right, where the lower border coincides with the right costal margin, but it extends as a wedge to the left of the midline between the anterior surface of the stomach and the left dome of the diaphragm. The liver is invested with peritoneum except on the posterior surface, where the peritoneum reflects onto the diaphragm, forming the right and left triangular ligaments. The posterior surface of the liver is triangular in outline, with its base to the right, and here the liver lying between the upper and lower leaves of the triangular ligaments is bare and devoid of peritoneum. Anteriorly, the convex surface of the liver lies against the concavity of the diaphragm and is attached to it by the falciform ligament, left triangular ligament, and upper layer of the right triangular ligament (Fig. 1-1).
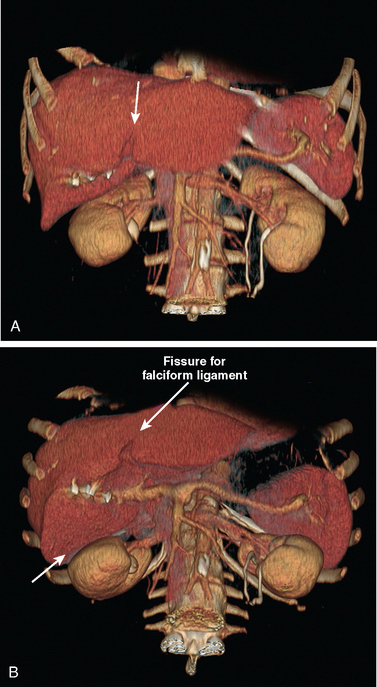
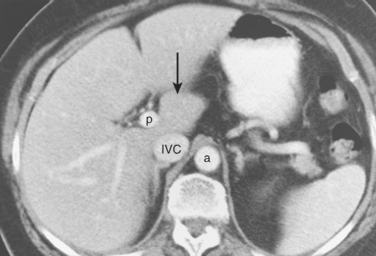
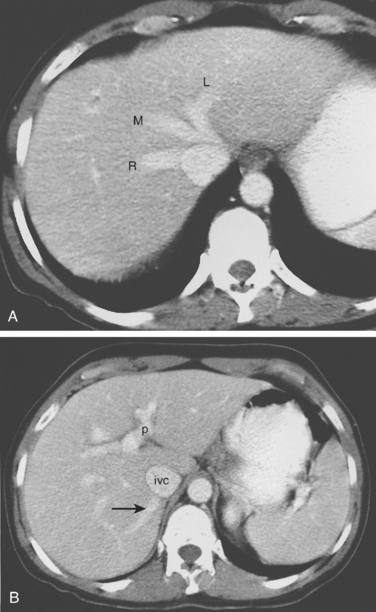
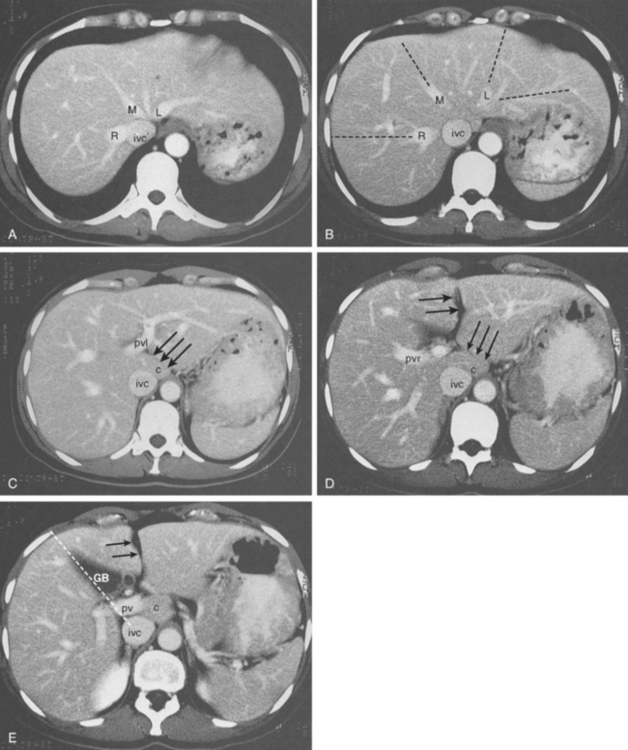
Behind the liver, the inferior vena cava (IVC) is embraced in a groove on its posterior surface (Figs. 1-2 and 1-3). The right adrenal vein is a short vessel that enters the IVC behind the bare area (see Fig. 1-2). Usually there are no vena caval tributaries posteriorly.
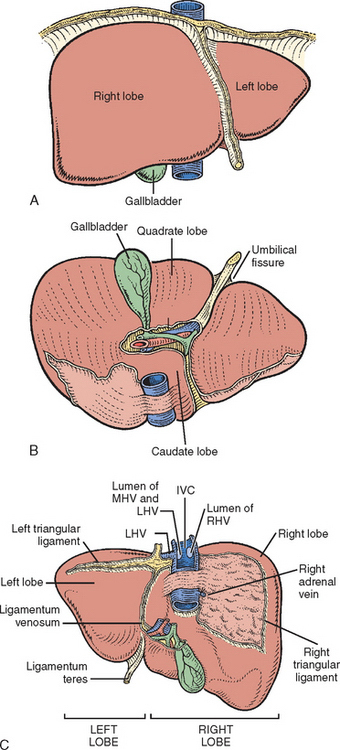
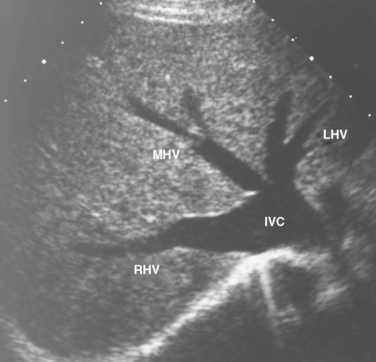
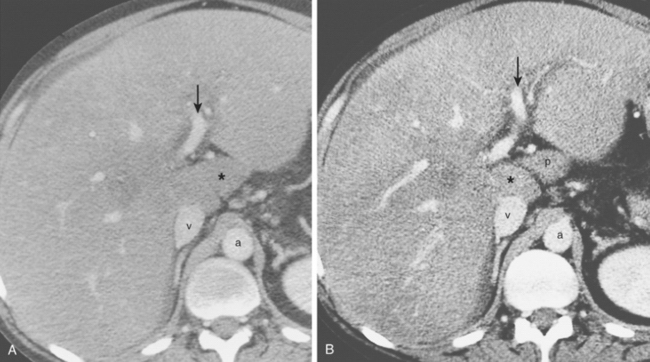
The hepatic veins (Figs. 1-4 and 1-5) drain directly from the upper part of the posterior surface of the liver at an oblique angle directly into the vena cava. The right hepatic vein, which is larger than the left and middle hepatic veins, has a short extrahepatic course of approximately 1 cm. The left and middle hepatic veins may drain separately into the IVC, but usually they are joined after a short extrahepatic course to form a common venous channel approximately 2 cm long that traverses to the left of the anterior surface of the IVC below the diaphragm (see Figs. 1-4 and 1-5). There are other hepatic veins in addition to the three major hepatic veins. The umbilical vein is single, in most cases, running beneath the falciform ligament between the middle and left hepatic veins and emptying into the terminal portion of the left hepatic vein. Additional posterior and inferior draining hepatic veins with a short course into the anterior surface of the IVC are frequent and may be large (Figs. 1-5 to 1-7).
FUNCTIONAL SURGICAL ANATOMY
The internal architecture of the liver is composed of a series of segments combining to form sectors separated by scissurae containing the hepatic veins (Fig. 1-8). The internal structure has been clarified by the publications of Goldsmith and Woodburne (1957), Couinaud (1957), and Bismuth and colleagues (1982). The description by Couinaud is the most complete and the most useful for the operating surgeon, and this description is generally used in this book.
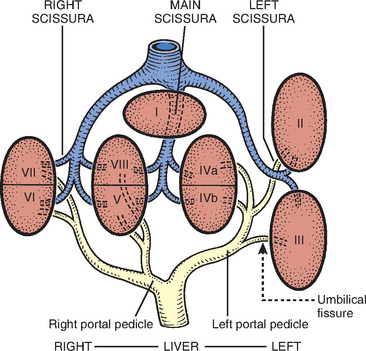
Essentially, the three main hepatic veins within the scissurae divide the liver into four sectors, each of which receives a portal pedicle. The main portal scissura contains the middle hepatic vein and progresses from the middle of the gallbladder bed anteriorly to the left of the vena cava posteriorly. The right and left parts of the liver, demarcated by the main portal scissura, are independent in terms of portal and arterial vascularization and of biliary drainage (Fig. 1-9). These right and left livers are themselves divided into two by the remaining portal scissurae. These four subdivisions in Couinaud’s nomenclature, (1957) are termed sectors (see Figs. 1-8 to 1-10).
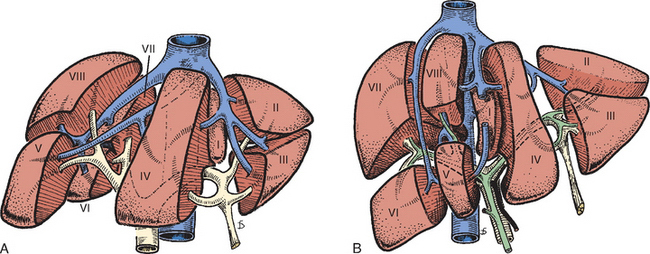

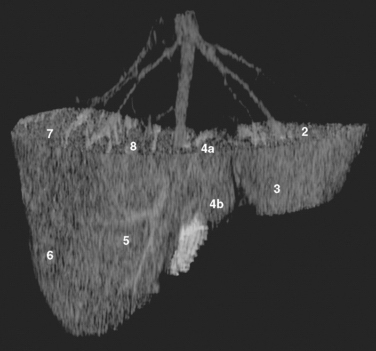
Figure 1-10 Corrosion cast of the segmental anatomy of the liver.
(Courtesy of Dr. B. Kekis, Athens, Greece.)
The right portal scissura separating the right liver into two sectors—anteromedial or anterior and posterolateral or posterior—is almost in the frontal plane with the body supine. The right hepatic vein runs within the right scissura. The left portal scissura divides the left liver into two sectors. The left portal scissura is not within the umbilical fissure because this fissure is not a portal scissura and contains a portal pedicle. The left portal scissura is located posterior to the ligamentum teres and within the left lobe of the liver along the course of the left hepatic vein. The anterior sector of the left liver is composed of a part of the right lobe (segment IV) that is to the left of the main portal scissura and of the anterior part of the left lobe (segment III) (see Figs. 1-8 to 1-10). The left posterior sector is the only sector composed of one segment (segment II) (Fig. 1-11).
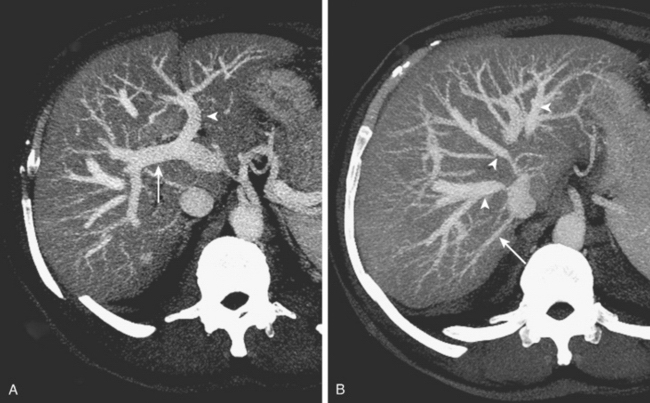
At the hilus of the liver, the right portal triad pursues a short course before entering the substance of the right liver (Figs. 1-6 and 1-12). In some cases, the right anterior and posterior pedicles arise independently, and their origins may be separated by 2 cm (Figs. 1-12 and 1-13). Indeed, it may appear as though the left portal vein arises from the right anterior branch (see also Fig. 1-48) On the left side, however, the portal triad crosses over approximately 3 to 4 cm beneath the quadrate lobe embraced in a peritoneal sheath at the upper end of the gastrohepatic ligament and separated from the undersurface of the quadrate lobe (segment IV) by connective tissue (hilar plate). This prolongation of the left portal pedicle turns anteriorly and caudally within the umbilical fissure giving branches of supply to segments II and III and recurrent branches to segment IV (see Figs. 1-8, 1-9, 1-14, and 1-15). Beneath the quadrate lobe, the pedicle is composed of the left branch of the portal vein and the left hepatic duct, but it is joined at the base of the umbilical fissure by the left branch of the hepatic artery.
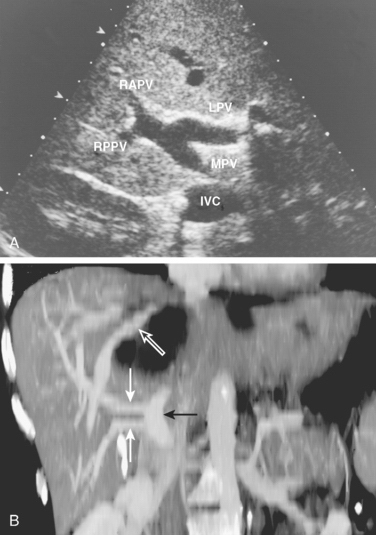
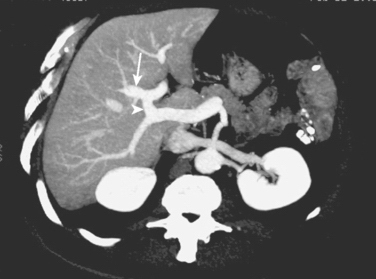
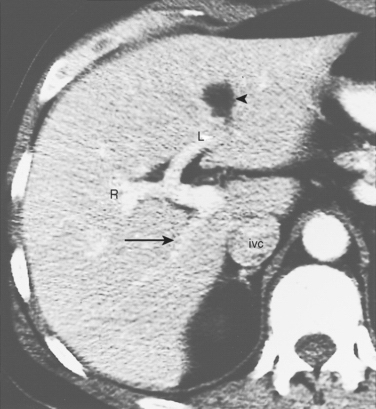
Figure 1-48 CT of common variant of portal vein branching. The right posterior portal vein (arrow) has a separate early origin from the main portal vein. The right anterior sectoral portal vein (R) and the left main portal vein (L) share a common trunk. Fissure of the ligamentum teres is seen anteriorly (arrowhead) (see also Figs. 1-12 and 1-46).

The branching of the portal pedicle at the hilus (Figs. 1-8, 1-12, 1-14, and 1-15), the distribution of the branches to the caudate lobe (segment I) on the right and left side, and the distribution to the segments of the right (segments V-VIII) and left (segments II-IV) hemilivers follow a remarkably symmetric pattern and allow separation of segment IV into segment IVa superiorly and segment IVb inferiorly (see Fig. 1-8). This arrangement of subsegments mimics the distribution to segments V and VIII on the right side. The umbilical vein provides drainage of, at least, parts of segment IVb after ligation of the middle hepatic vein and is important in the performance of segmental resection.
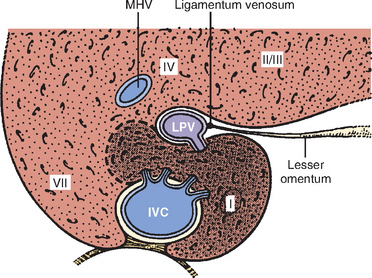
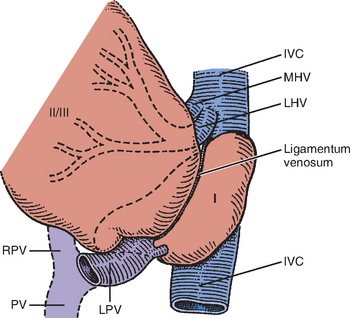
The caudate lobe (segment I) is the dorsal portion of the liver lying posteriorly and embracing the retrohepatic IVC. The lobe lies between major vascular structures. On the left, the caudate lies between the IVC posteriorly and the left portal triad inferiorly and the IVC and the middle and left hepatic veins superiorly (Figs. 1-16 and 1-17). The portion of the caudate on the right varies, but is usually quite small. The anterior surface within the parenchyma is covered by the posterior surface of segment IV, the limit being an oblique plane slanting from the left portal vein to the left hepatic vein. Thus, there is a caudate lobe (segment I) with a constantly present left portion and a right portion of variable size (see Figs. 1-16 and 1-17).
The posterior edge of the caudate lobe on the left has a fibrous component, which fans out and attaches lightly to the crural area of the diaphragm, but extends posteriorly behind the vena cava to link with a similar component of fibrous tissue from the posterior surface of segment VII and embraces the vena cava (see Figs. 1-2C and 1-16). This ligament may be replaced, in whole or in part, by hepatic tissue, and the caudate may completely encircle the IVC and contact segment VII on the right side. A papillary process of the caudate lobe can be mistaken for an enlarged lymph node on computed tomography (CT) scan (Fig. 1-18). To summarize:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


