Fig. 1.1
The intrathoracic location of the liver and the inferior location of the right kidney. 4–10 indicate rib numbers
The protected position of the liver in the recesses of the right upper quadrant mandates complete liberation of the liver from its peritoneal attachments for adequate exposure and visualization of hepatic injuries. The peritoneal attachments include the falciform ligament, coronary ligament, triangular ligaments, and the hepatogastric ligament. The coronary and triangular ligaments essentially suspend the liver from the parietal peritoneum superiorly and enclose the bare area of the liver, which lies at the apex of the organ (Fig. 1.2).

Fig. 1.2
The ligamentous attachments of the liver and the enclosed bare area. Arrow shows direction of mobilization, would leave un-labeled.
The Glissonian capsule surrounds the liver parenchyma and extends to envelope the portal triad as it enters the liver consisting of the portal vein, the hepatic artery, and the bile duct. The portal vein lies deepest in the triad, with the hepatic duct normally occupying the superficial lateral position and the artery the superficial medial position. A fibrous sheath of connective tissues envelopes the triad at the hepatic hilum and is referred to as the hilar plate, which lies in continuity with the cystic and umbilical plates and acts as a protective barrier for the extrahepatic triad.
Segmental Anatomy
Many have contributed to our current understanding of hepatic anatomy, though most credit Claude Couinaud’s 1954 work, Lobes et segments hepatiques, with the definitive documentation of hepatic segmental anatomy and the standardization of segmental terminology. Couinaud’s descriptions were unique as they were based on anatomic relationships to the main portal vein and its branches, as the variability of portal vein anatomy is much less than that of the hepatic artery or duct.
Couinaud described three levels of the liver: the right and left hemi-livers, the sectors, and the segments. The portal vein bifurcation into right and left branches divides the liver into its right and left hemi-livers, as based on portal venous blood supply.
Further division of the right and left portal veins divides the right and left lobes of the livers into sectors; two are present on the right and two on the left. The right hemi-liver is divided into anterior and posterior sectors. The posterior sector consists of segments VI and VII, and the right anterior sector consists of segments V and VIII.
The left portal vein divides into two branches, one to segment II and one to segments III and IV. Thus, the left hemi-liver consists of a lateral sector (segment II) and a paramedian sector (segments III and IV), which are separated by the falciform and round ligaments. Segment I, or the caudate lobe, lies posterior to the right hemi-liver and between the portal vein bifurcation and vena cava with its own hepatic venous drainage and portal venous tributary (Fig. 1.3).
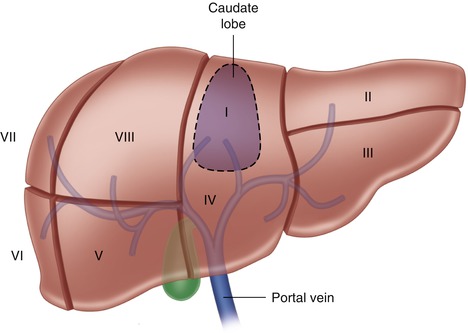
Fig. 1.3
The segmental nature of the liver and relationship to the portal vein
Couinaud further described the suprahepatic sectoral anatomy and its relationships to the right, middle, and left hepatic venous drainage. The course of the portal venous division overlaps with the hepatic venous drainage and thus helps define the eight portal segments and their drainage pattern.
Hepatic Arterial Anatomy
Hepatic arterial anatomy is well recognized for its multiple variations and their surgical implications in hepatic surgery. Recognition of these anatomic variations is critical when pursuing operative intervention for traumatic liver injury, as indiscriminate ligation can lead to hepatic ischemia and necrosis.
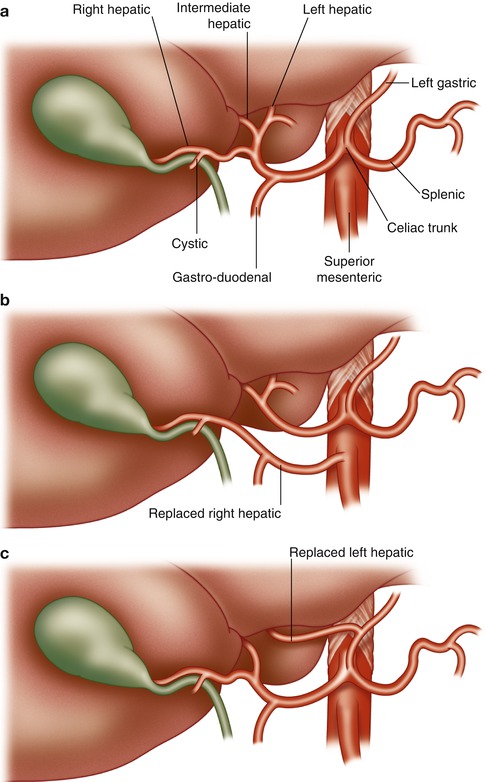
The most common variant involves the common hepatic artery originating from the celiac trunk prior to its division into hepatic artery proper and gastroduodenal artery. The proper hepatic artery then continues its course toward the hilum of the liver before bifurcating into the right and left hepatic arteries within the hilar plate.
The next two most common variants consist of the replaced or accessory origins of the right and left hepatic arteries. Replaced arteries act as the sole blood supply to its equivalent hemi-liver and accessory arteries act as an additional source of arterial blood. Replaced or accessory right hepatic arteries originate from the superior mesenteric artery and can be found intraoperatively by the presence of an arterial pulse along the lateral border of the hepatoduodenal ligament. Replaced or accessory left hepatic arteries originate from the left gastric artery and manifest as an arterial pulse in the lesser omentum (Fig. 1.4). Less common anomalies include double-replaced patterns, common hepatic arterial derivation from the superior mesenteric artery, and common hepatic artery origin directly from the aorta, among others.
 Acquisition of Surgical Skills by Hepatobiliary Rotation
Acquisition of Surgical Skills by Hepatobiliary Rotation
 Parenchyma: Formal Lobectomy
Parenchyma: Formal Lobectomy
 Massive Hepatic Hemorrhage: Identification
Massive Hepatic Hemorrhage: Identification
 Damage Control Laparotomy
Damage Control Laparotomy
 Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
 Acquisition of Surgical Skills in Animal and Simulation Laboratories
Acquisition of Surgical Skills in Animal and Simulation Laboratories




Fig. 1.4
(a) The most common variant of hepatic arterial supply, (b) replaced right hepatic artery, and (c) replaced left hepatic arterial variants
Related posts:
Acquisition of Surgical Skills by Hepatobiliary Rotation
Parenchyma: Formal Lobectomy
Massive Hepatic Hemorrhage: Identification
Damage Control Laparotomy
Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
Acquisition of Surgical Skills in Animal and Simulation Laboratories
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
