Fig. 16.1
Child arranged in the Galdakao-modified supine Valdivia position with reference lines for the renal puncture
16.4 Obese Patients
Obesity has been identified as an independent risk factor for stone formation in the United States. Obesity (BMI >35) also places surgical patients at a greater risk of complications, because of the increased incidence in this group of diabetes, hypertension, ischemic heart disease, postoperative deep venous thrombosis, and pulmonary embolism and because of poor radiographic visualization, obscure anatomic landmarks, more difficult renal access, and inferior stone-free rates [15].
Because of a greater perceived difficulty in performing percutaneous surgery in obese patients, investigators have theorized in the past that PNL in such patients may be less effective, technically difficult, and associated with higher complication rates [16]. On the contrary, there are no adverse effects of obesity on PNL outcomes in terms of stone-free rates, complication rates, and length of hospital stay [17–19], apart from a slightly longer operative time [20]. Therefore, morbid obesity is no sufficient reason for choosing multisession retrograde endoscopic lithotripsy instead of PNL for the treatment of large renal calculi, obtaining low stone-free rates as 33 % [21].
We agree that there are some tips and tricks and modifications of the standard PNL technique and instrumentation to bear in mind when planning a PNL in an obese patient [17, 22], like the use of larger and longer access sheaths and nephroscopes as effective additions to the urologist’s armamentarium, the suture of the Amplatz sheath to the skin to prevent its loss beneath it or the muscle fascia, and the trick to pull abdominal fat opposite to the operated side, possibly putting the patient in the supine/supine-modified position.
Supine PNL has been proven to be very ergonomic and suitable in obese patients (Fig. 16.2), also considered high-risk ones for the abovementioned reasons. The supine decubitus has the advantages of a significant shorter operative time (the 2008 CROES study reported the opposite, with the bias that they did not take into account all the preliminary retrograde procedure before puncturing the kidney) and hospital stay [5, 20, 23–25].

Fig. 16.2
Obese patient in the Galdakao-modified supine Valdivia position, ready for ECIRS (a) and prepared with adhesive strips in order to move the fat towards the side that does not need to be operated (b)
16.5 Skeletal Malformations
Scoliosis involves a lateral and rotational deformity of the thoracolumbar spine and occurs in less than 4 % of the population, being 70 % idiopathic and 30 % secondary to congenital, neuromuscular disease, mesenchymal disorders, trauma, or infection.
PNL for urolithiasis in patients with spinal deformities, such as kyphoscoliosis or severe hip ankylosis, might be challenging from an anaesthesiological (respiration impaired, mainly restrictive pulmonary deficit), surgical (anatomic variations and accurate preoperative planning to avoid visceral damage), and technical point of view. A thorough preoperative imaging study should be carried out, especially to choose the best therapeutic approach and, in case of PNL, the more fit position [26]. The supine position improves anesthesiological assistance from a cardioventilatory point of view and implies less risk of postural damage, more comfort of the patient, and the possibility of a combined approach, although supine position may not be applicable to all skeletal malformations and may leave a very reduced space between ribs and iliac crest when the stone is located on the concave side of the spine (Fig. 16.3).
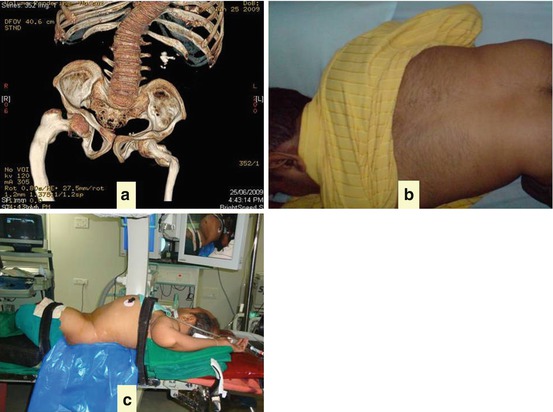
Fig. 16.3
Patient with kyphoscoliosis and osteogenesis imperfecta. CT scan for the study of the staghorn urolithiasis and of the anatomy (a) It was impossible to put the patient in the prone position (b) and thus the supine position was employed (c)
16.6 Previous Surgery
Urolithiasis has been often previously treated by means of extracorporeal shock wave lithotripsy (ESWL) and percutaneous, ureteroscopic, open, or laparoscopic surgery [27, 28]. Given the equivalence prone/supine, safe and effective PNL can be performed in such patients, with no higher risk of complications, except the need for more attempts to access the pelvicalyceal system and the difficulty in tract dilation secondary to fascial and retroperitoneal scarring (and in this case the use of Alken coaxial dilators is of the utmost importance) [29] (Fig. 16.4).

Fig. 16.4
Post-pyelolithotomy scar in a patient undergoing ECIRS
16.7 Bilateral Urolithiasis

16.8 Upper Pole Puncture
During ECIRS performed in the Galdakao-modified supine Valdivia position, upper pole puncture is seldom required because of the use of flexible antegrade/retrograde endoscopes. Under this respect, a patient suffering from upper calyceal stone disease is the ideal one for ECIRS in this position.
In any case, if a subcostal access to the renal superior calyx is required in a supine position, renal displacement technique should be carried out, with lung inflation to facilitate the puncture and to reduce intrathoracic morbidity. Alternatively, the kidney could be pulled down with a balloon catheter [32], or, according to our personal experience, the inclination of the patient on the operating table can be further increased.
16.9 Urinary Congenital Malformations
A variety of developmental abnormalities of the kidney can present in adulthood. Anomalous kidneys (solitary, horseshoe, ectopic, and malrotated kidneys) often have abnormal renal position, anatomy, calyceal orientation, relationships of the calyces to the renal pelvis and upper ureter, rotation, aberrant vasculature, relative renal immobility, atypical relationships between kidney and other organs, and all elements causing urinary stasis with stone formation, often associated with concomitant infection and metabolic alterations. The same reasons causing an increased risk of stone formation contribute to an increased risk of renal stone management in anomalous kidneys [7, 33, 34].
PNL in anatomically abnormal kidneys is challenging for fear of inaccessibility, and of vascular and visceral injury, but can be safely and effectively performed, sometimes with an extended operative time. Even more than usual it deserves a meticulous preoperative assessment of the anatomy of the collecting system and of visceral relationships for planning an optimal renal puncture, intraoperatively aided by real-time ultrasound assistance. The supine and oblique positions may be particularly favorable, especially in ectopic pelvic and malrotated kidneys [35, 36], with the bolster below the hemipelvis pushing the kidney closer to the anterior abdominal wall, while the bowel loops are displaced cephalad both by the position and by the pressure of the ultrasound probe itself. Also in horseshoe kidneys (Fig. 16.6), the supine position may be particularly useful to improve safety and efficacy of the percutaneous procedure. All the same, universal application of PNL may also be challenged with alternative and creative solutions, like the combination with the laparoscopic approach (personal experience) (Fig. 16.7) or the alternative use of single port laparoscopic access for pyelolithotomy surgery [37, 38].
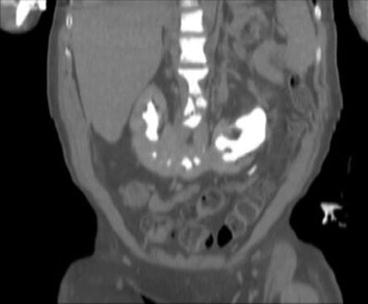
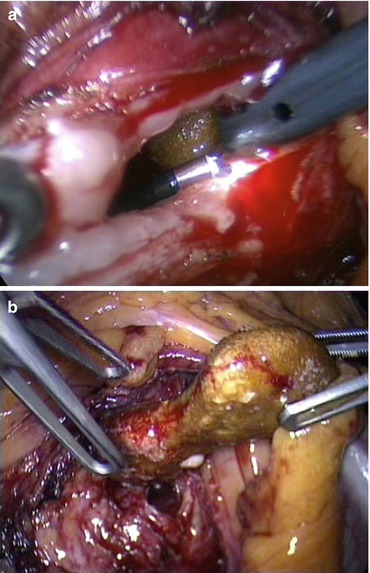
Fig. 16.6
CT scan without contrast of a paraplegic patient with a horseshoe kidney
Fig. 16.7
Combination of laparoscopy and ECIRS in the same paraplegic patient. Flexible RIRS phase (a) and litholapaxy (b)
As to UPJ stricture, similar to what happens in pediatric patients, concomitant laparoscopic correction should be performed; thus, associated stones, often candidates to a percutaneous approach, may be extracted during the laparoscopic procedure, with graspers or combining trans-trocar lithotripsy. This is also our personal experience.
16.10 Transplanted Kidney
Nephrolithiasis is an unusual (0.2–3 % of all urological complications) but challenging late complication of transplanted kidneys, due to hyperparathyroidism and nonabsorbable sutures, as well as to other predisposing causes identical to patients with native kidneys (obstructive uropathy, recurrent urinary tract infections, metabolic abnormalities like hyperuricosuria).
Renal stones in transplanted kidneys need prompt recognition and management, as they can be an important cause of deterioration of the graft function. PNL is most often the best modality to render patients stone-free, being effective and safe. Allograft superficial location close to the skin and its proximity to the bony pelvis, peritoneum, and iliac vessels makes the supine position a valid option, also allowing combined antero-retrograde approach with the use of flexible scopes [39–42].
16.11 After Urinary Diversions
Complications related to urinary-intestinal diversions are numerous and rather frequent (up to 11 % within 3 years after surgery) because of anatomic and metabolic factors including refluxing ureteroileal anastomoses, upper urinary tract dilation, urinary stasis, and heightened risk of stone formation. The hyperchloremic metabolic acidosis from reabsorption of solutes across the intestinal mucosa results in an increased burden of urinary titratable acids, with an increased risk of hyperoxaluria, calcium oxalate stone formation in patients with ileal resection, and higher recurrence of urinary tract infections. Urea-splitting organisms elevate urinary pH and increase the risk of forming calcium phosphate and struvite stones [43]. Renal and ureteral calculi may be approached antegradely or with a combined approach, if the ureteroileal anastomosis is compliant enough to allow a retrograde approach [44], being the supine position particularly beneficial in this setting.
16.12 Pregnancy
Normal anatomic and physiological changes of the urinary tract during pregnancy (mechanical compression of the ureter, effect of the circulating progesterone on the ureteral smooth muscle with reduced peristalsis and increased dilation, gestational hypercalciuria secondary to a combination of increased GFR, dietary and fetal factors) may predispose to stone formation. Thus, nephrolithiasis is a not infrequent complication in pregnancy (the incidence of symptomatic nephrolithiasis during pregnancy varies between 1 in 244 and 1 in 2,000 pregnancies, but the actual incidence is likely to be higher), representing a clinical dilemma because of potential risks to both mother and fetus [45].
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


