Fig. 14.1
Laser vaporization of a stone (high frequency and low energy)

Fig. 14.2
Laser fragmentation of a stone (low frequency and high energy)
The second one aims at obtaining bigger pieces with a pneumatic device until reaching a diameter allowing their passage through the Amplatz sheath (Fig. 14.3). “Single pulse setting” has been found more efficient to obtain such a controlled stone disintegration. Reportedly, this latter method allows to obtain better stone free rates because it prevents small fragments to migrate into unreachable parts of the collecting system [1].

Fig. 14.3
Ballistic fragmentation of a stone in large fragments
14.3 Stone Factors
14.3.1 Stone Hardness
14.3.1.1 Soft Stones
Soft stones like struvite (magnesium ammonium phosphate) or weddellite (calcium oxalate dihydrate) respond well to pulverization with ultrasound. They are quickly transformed into sand and aspirated through the ultrasound probe. To increase fragmentation efficacy, ultrasound can be combined with simultaneous ballistic lithotripsy, like in the LithoClast Master device or potentiated like in the CyberWand device. However, the large 10 Ch ultrasound probes necessitate nephroscopes with a larger working channel, allowing not only the passage of the probe but also a sufficient irrigation flow.
An abundant irrigation is crucial, especially in the supine position: in fact, due to the roughly horizontal or downward axis of the Amplatz sheath (see Chap. 13) and to the efficient aspiration, the collecting system tends to collapse and visibility deteriorates. To guarantee a high flow, the irrigation fluid containing bag should be elevated (Fig. 14.4). Alternatively, some urologists use hyperpressurized irrigation or peristaltic pumps to increase irrigation flow, although continuous or intermitted high intrarenal pressures should be avoided in order to prevent the uroseptic risk more marked in case of infectious stones.

Fig. 14.4
Elevation of the fluid bags in order to increase the irrigation pressure
14.3.1.2 Hard Stones
Hard stones such as whewellite (calcium oxalate monohydrate), cystine, or brushite (calcium phosphate) respond poorly to ultrasonic fragmentation. Pneumatic lithotripters (Swiss LithoClast) or combination of pneumatic and ultrasound (like Swiss LithoClast Master) is recommended. The CyberWand device uses only ultrasound, but due to the two different frequencies, its efficacy is similar to that of the LithoClast Master. Recently, a compact, autonomous, and cordless handheld lithotripter has also been developed. The StoneBreaker is highly efficient in case of hard stones because it produces a high amount of pressure (31 bar, compared with the 3 bar of standard pneumatic lithotripters) and despite the high energy of the mechanical shock minimal displacement at the tip of the probe [2, 3].
14.3.2 Location
As previously mentioned, the nephrostomy tract should pass through a calyx that allows dealing with the major stone burden. In this case, rigid and straight fragmentation tools such as ultrasound or pneumatic or combined lithotripters can be used.
However, in case of complex or multiple calculi, not all calyces can be reached with the rigid nephroscope. In such circumstances, if multiple percutaneous tracts are not a routine choice, a flexible nephroscope via the Amplatz sheath (Fig. 14.5a) or a transurethrally passed uretero-nephroscope (Fig. 14.5b) should be used. Obviously, such instruments necessitate the use of laser fiber technology, to be employed in situ or to help stone dislocation into more reachable locations by means of a basket.
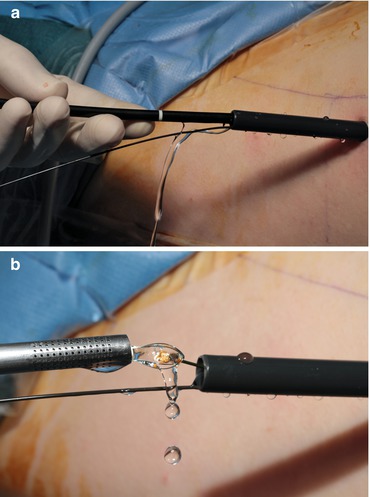
Fig. 14.5
For complex urolithiasis flexible nephroscope (a) or flexible ureteroscope (b) are fundamental aids for a better stone clearance
14.3.3 Stone Size and Burden
Staghorn stones necessitate a specific fragmentation strategy. A step-by-step description was recently given by Peter Alken for prone PNL [4] (Fig. 14.6). This method is also valid for supine position, with the difference that in the latter the whole procedure can be assisted by retrograde ureteroscopic laser fragmentation of stone portions difficult to reach with the rigid nephroscope.
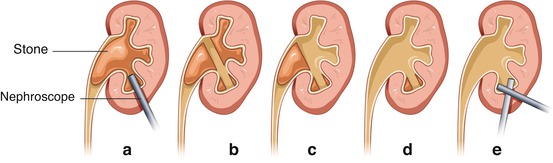
Fig. 14.6




(a) Start fragmentation in the puctured calix except laterally because of the risk of injury to forniceal veins. (b) Carry on fragmentation until the medial wall of the kidney pelvis is reached. (c) Clear distant calices. The fragment in the ureteropelvic junction prevents fragment migration into the ureter. (d) Remove the remaining stone from the ureteropelvic junction. (e) Complete fragment extraction in the punctured calix in the forniceal region. Lithotripsy strategy (courtesy of professor Peter Alken) for a staghorn stone (© Carole Fumat)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
