Operative steps
Degree of technical difficulty (scale 1–10)
1. Port placement and exploratory laparoscopy
3
2. Identification and mobilization of bowel
4
3. Exteriorization of bowel
2
4. Ostomy maturation
1
Port Placement and Exploratory Laparoscopy
A 2.5-cm incision is made in the right lower quadrant at the predetermined ileostomy site. The incision is carried down to the anterior rectus sheath, which is then divided in a cruciate fashion. The skin and subcutaneous fat are excised as a cone of tissue down to the anterior rectus sheath (see Fig. 24.1). The rectus abdominis muscle is spread in the direction of its fibers exposing the posterior rectus sheath and peritoneum (see Fig. 24.2) which are also divided in a cruciate fashion over a distance of 2.5 cm, wide enough to accommodate two fingers. The single-port access system (see Figs. 24.3 and 24.4) is then inserted through this incision. The abdomen is insufflated with CO2 to 15 mmHg. A 5-mm laparoscope with a flexible steerable tip is used to visualize the abdomen. Single-incision laparoscopic instruments may be used, but standard laparoscopic instruments are suitable in most cases.

Fig. 24.1
Anterior fascia
Fig. 24.2
Posterior fascia
Fig. 24.3
Triport
Fig. 24.4
Triport placed
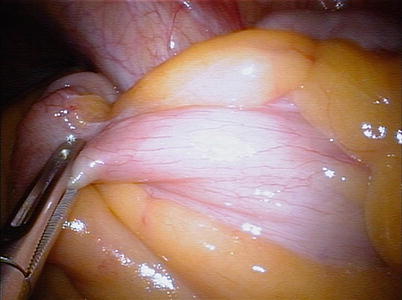
Identification and Mobilization of Bowel
The terminal ileum is located, and a point on the small bowel about 15–20 cm proximal to the ileocecal valve is identified laparoscopically. Visualization of the ligament of Treves, located on the antimesenteric border of the terminal ileum just proximal to the ileocecal valve, is also helpful in identifying the anatomy (see Video 24.1 and Fig. 24.5) [2]. The terminal ileum is inspected for any pathology as well as length of mesentery available for loop stoma creation. The proximal side (one serosal thermal burn) and distal side (three serosal thermal burns) of this point on the small bowel are marked by using laparoscopic electrocautery [1] (see Video 24.2 and Fig. 24.6). The bowel should be marked close to the ileocecal valve if the stoma is permanent. On the other hand, if the stoma is temporary, the bowel should be marked at least 15 cm proximal to the ileocecal valve to facilitate subsequent closure. Alternatively, the future ileostomy site may be marked with different colored sutures for orientation [2]. If the procedure involves a creation of a laparoscopic sigmoid colostomy, the white line of Toldt is mobilized as needed [2]. When an end stoma is indicated, intracorporeal mesenteric division may be performed either with laparoscopic clips or an endoscopic vascular linear stapler, if necessary [5, 6].
 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Robotic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
 Transanal Endoscopic Surgery (TES)
Transanal Endoscopic Surgery (TES)
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach
 Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach




Related posts:
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
Transanal Endoscopic Surgery (TES)
Proctectomy: Total Robotic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
