Squamous Lesions
SQUAMOUS METAPLASIA
Squamous epithelium, particularly in the area of the trigone, is a common finding in women (Fig. 9.1) (also see Chapter 1). Trigonal squamous epithelium in women represents a normal histologic variant occurring under hormonal influence, unassociated with local injury. Under other conditions, elsewhere in the bladder, squamous epithelium resulting from the metaplasia of urothelium can undergo keratinization and may exhibit parakeratosis, hyperkeratosis, and even acquire a granular layer (Fig. 9.2). This metaplastic epithelium is not preneoplastic per se, but under some circumstances, especially when extensive and involving large regions of the bladder it may lead to squamous carcinoma (1). This is the sequence of events, for example, in patients with long-standing schistosomiasis of the urinary bladder or, in the case of squamous carcinoma, arising in bladder diverticula (2, 3, 4). In these cases, it may be possible to observe keratinizing squamous metaplasia adjacent to in situ and invasive squamous carcinoma. The pathologist is obligated to mention the presence and extent of keratinizing squamous metaplasia in a transurethral biopsy specimen. Khan et al. (5) described their experience with 34 patients with keratinizing squamous metaplasia. Although the extent of involvement correlated with subsequent risk of carcinoma, any degree of keratinizing squamous metaplasia is a significant risk factor for the development of subsequent carcinoma as well as other complications such as bladder contracture and obstruction.
VERRUCOUS SQUAMOUS HYPERPLASIA
Verrucous squamous hyperplasia consists of a spiking or church spirelike squamous hyperplasia (Fig. 9.3). Marked hyperkeratosis, parakeratosis, and elongation of the rete pegs are also present, but the lesions lack the broad invasive tongues seen with verrucous carcinoma. Although this lesion has only been relatively recently reported in the urinary bladder, verrucous squamous hyperplasia is well recognized in the oral cavity and upper respiratory tract. In these sites, verrucous squamous hyperplasia is an irreversible lesion with a considerable risk for evolving into verrucous or other forms of squamous cell carcinoma. In a study of this lesion in the bladder, clinical follow-up information was available in five cases
of verrucous squamous hyperplasia (6). One developed conventional invasive squamous cell carcinoma and another patient was subsequently diagnosed with urothelial carcinoma in situ (CIS). These results suggest that verrucous squamous hyperplasia may represent a premalignant lesion or may be associated with premalignant lesions in the bladder, and should be treated and followed up accordingly. In a series of invasive squamous cell carcinoma, 7% of patients had squamous hyperplasia in background mucosa (7).
of verrucous squamous hyperplasia (6). One developed conventional invasive squamous cell carcinoma and another patient was subsequently diagnosed with urothelial carcinoma in situ (CIS). These results suggest that verrucous squamous hyperplasia may represent a premalignant lesion or may be associated with premalignant lesions in the bladder, and should be treated and followed up accordingly. In a series of invasive squamous cell carcinoma, 7% of patients had squamous hyperplasia in background mucosa (7).
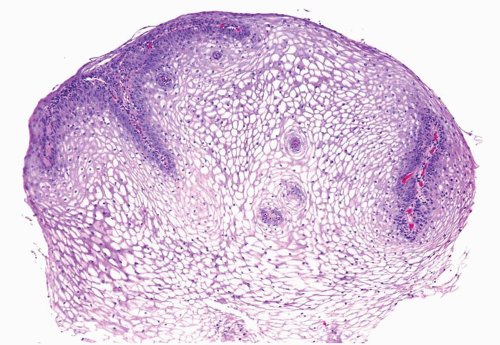 FIGURE 9.1 Glycogenated squamous metaplasia. |
CONDYLOMA ACCUMINATA
Condyloma acuminata are common sexually transmitted benign tumors caused by a human papillomavirus (HPV) (Figs. 9.4, 9.5) (efigs 9.1-9.7).
They occur most frequently on the mucocutaneous surfaces of the external genitalia, perineum, and anus but extension into the urethra is not uncommon, occurring in up to 20% of cases. On rare occasions, they may involve the bladder or even the ureters (6, 8, 9, 10). Most patients have associated extensive condyloma of the external genitalia. Isolated condyloma of the bladder often presents in immunosuppressed patients. Of the three cases of condyloma of the bladder reported by Del Mistro et al. (11), two occurred in immunocompromised patients. The three patients reported by
Cheng et al. (12) were all associated with extensive condyloma in the external genitalia, and one of the patients had follow-up studies showing multiple recurrence of condyloma. Condylomas of the bladder are refractory to conservative treatment and are prone to multiple recurrences (11). There are also multiple case reports of condylomas in the urinary bladder associated with high-grade dysplasia, squamous, verrucous, or urothelial bladder cancer, warranting close follow-up of patients with bladder condylomas (6, 7, 13, 14). If one has as a differential diagnosis, squamous papilloma versus condyloma of the bladder, in situ hybridization for low- and high-risk HPV may be performed, which will only be positive in condylomas.
They occur most frequently on the mucocutaneous surfaces of the external genitalia, perineum, and anus but extension into the urethra is not uncommon, occurring in up to 20% of cases. On rare occasions, they may involve the bladder or even the ureters (6, 8, 9, 10). Most patients have associated extensive condyloma of the external genitalia. Isolated condyloma of the bladder often presents in immunosuppressed patients. Of the three cases of condyloma of the bladder reported by Del Mistro et al. (11), two occurred in immunocompromised patients. The three patients reported by
Cheng et al. (12) were all associated with extensive condyloma in the external genitalia, and one of the patients had follow-up studies showing multiple recurrence of condyloma. Condylomas of the bladder are refractory to conservative treatment and are prone to multiple recurrences (11). There are also multiple case reports of condylomas in the urinary bladder associated with high-grade dysplasia, squamous, verrucous, or urothelial bladder cancer, warranting close follow-up of patients with bladder condylomas (6, 7, 13, 14). If one has as a differential diagnosis, squamous papilloma versus condyloma of the bladder, in situ hybridization for low- and high-risk HPV may be performed, which will only be positive in condylomas.
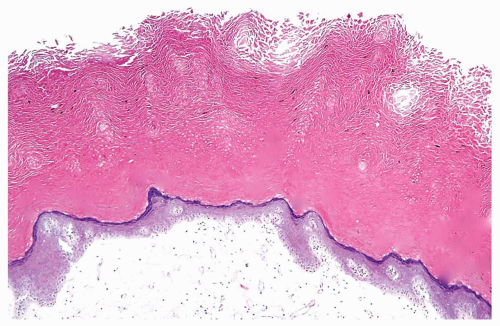 FIGURE 9.2 Keratinizing squamous metaplasia. |
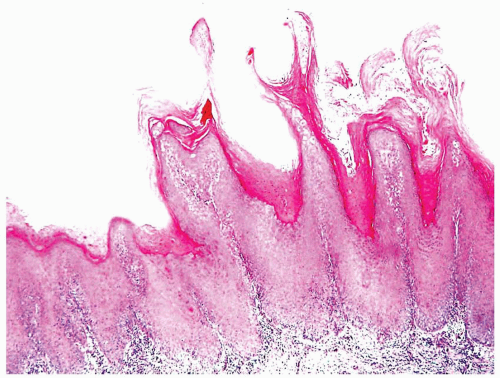 FIGURE 9.3 Verrucous squamous hyperplasia. |
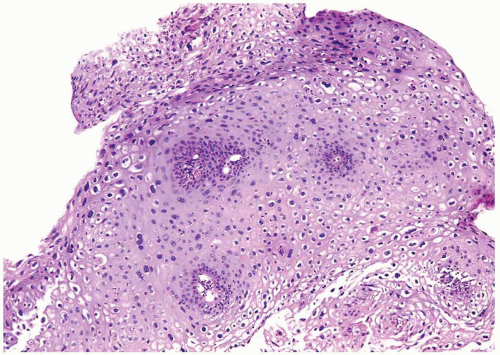 FIGURE 9.4 Condyloma acuminatum. |
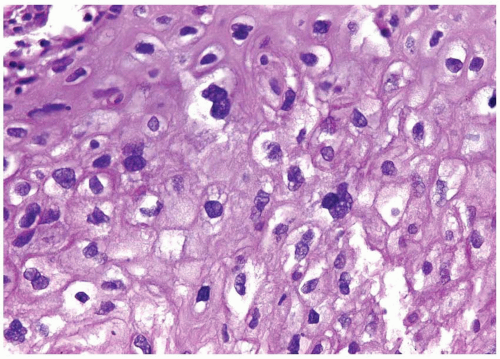 FIGURE 9.5 Condyloma acuminatum (higher magnification of Figure 9.4). |
SQUAMOUS PAPILLOMA
In 2000, Cheng et al. (12) described a series of seven cases of squamous papilloma, five occurring in the urinary bladder and the others in the urethra (Figs. 9.6, 9.7




Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
