(1)
Department of Vascular Surgery, Evangelisches Krankenhaus Königin Elisabeth Herzberge, Berlin, Germany
15.1 Renal Transplant Recipients
When creating a new AV access or before closing an access which is no longer required, special aspects need to be considered.
15.1.1 Creation of a New Vascular Access
Patients who are under long term glucocorticoid treatment may require an additional perioperative stress dose due to the suppression of the hypothalamic-pituitary-adrenal axis.
Transplanted patients have a higher risk for impaired wound healing and infections, and also sometimes increased propensity to bleed. The skin and blood vessels may be extremely friable, so that atraumatic surgical techniques, careful hemostasis, and extra cautious draping and placement of incise film if applicable are particularly important.
15.1.2 Request for the Closure of an AV Access
Many patients with a reliably stable transplant function inquire whether it is possible to ligate the AV access. Crucial aspects include:
Kidney graft function
Time passed since transplant surgery,
Biological age and general condition of the patient
Remaining options for future AV access surgery
Closure of the Vascular Access
We only close the vascular access if:
The kidney transplant function is good.
There are further possibilities for the creation of potential future accesses.
Frequency
Very rare.
Technical Hint
The continuity of the vein should be preserved if possible, so as to be able to use it for a potential future new vascular access. Illustrated examples are Fig. 15.1 which shows the closure of a cephalic fistula, and Fig. 15.2 that of an elbow fistula. Under certain circumstances the vein may remain patent due to the inflow from side branches.
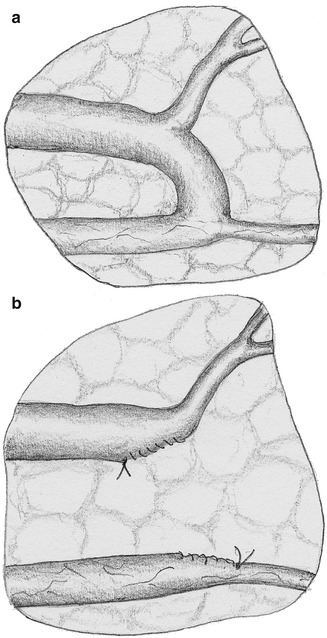
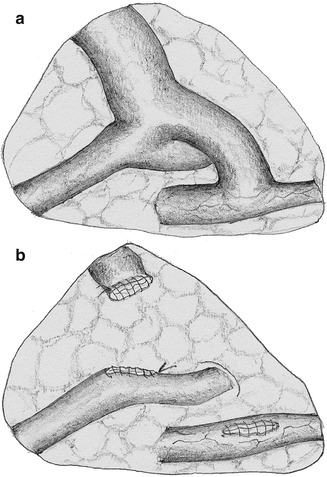
Fig. 15.1
Surgical occlusion of a cephalic forearm fistula while preserving the venous continuity. (a) Before. (b) After
Fig. 15.2
Surgical occlusion of an elbow AV fistula while preserving the continuity of the basilic vein. (a) Before. (b) After
Preservation of the Vascular Access with Flow Reduction
We try to preserve the vascular access if:
Options for future access surgery are limited
The patient is young
The procedure is different for AV fistulas and AV shunts.
AV Fistulas
Depending on the local situation there are the following options:
Perform flow reduction if there is an only slightly dilated vein (cf. Chap. 11).Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree








