Single-Incision Laparoscopic Total Abdominal Colectomy with End Ileostomy
KEY STEPS
1. Insertion of single-incision port, at ileostomy site previously marked by enterostomal therapist.
2. Laparoscopic mobilization of the right colon and the terminal ileum.
3. Laparoscopic mobilization of the transverse colon and takedown of the splenic flexure, with division of middle colic vessels.
4. Laparoscopic mobilization of the left colon.
5. Mobilization and division of the upper rectum, mesorectum, and descending colonic mesentery.
6. Specimen extraction and ileostomy through single-port site.
ADDITIONAL ADVICE
1. As only two instruments are in place, the direction of traction with the left-hand instrument is a little more toward the camera, as wide sweeping arcs of traction do not work well.
PATIENT POSITIONING
The patient is placed supine on the operating table on a bean bag. After induction of general anesthesia and insertion of an orogastric tube and a Foley catheter, the legs are placed in yellow fin stirrups. The arms are tucked at the patient’s side and the bean bag is aspirated (Fig. 19.1). The abdomen is prepared with antiseptic solution and draped routinely (Chapter 2).
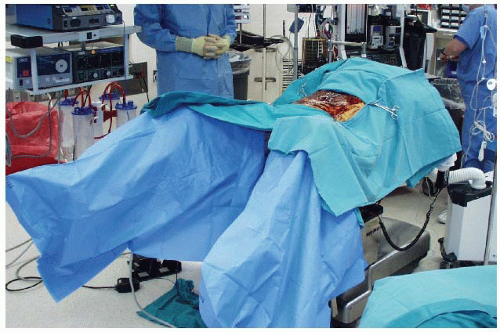 FIGURE 19.1. Patient positioning. |
INSTRUMENT POSITIONING
The primary monitor is placed on the right side of the patient at the level of the hip. The operating nurse’s instrument table is placed between the patient’s legs. There should be sufficient space to allow the operator to move from either side of the patient to between the patient’s legs if necessary. The primary operating surgeon stands on the left side of the patient with the assistant standing on the patient’s right side, and moving to the left side, caudad to the surgeon once ports have been inserted. A long 30-degree, 5-mm camera lens is used.
SINGLE-PORT INSERTION
The insertion of the single port is performed through a 2.5-cm incision using a modified Hasson approach at the ileostomy site (Chapter 3). A circular 2.5 cm incision is made. This is deepened down to the linea alba, which is then grasped using Kocher clamps. Cautery is used to open the fascia between the Kocher clamps and Kelly forceps are used to open the peritoneum bluntly, and a 2.5-cm fascial incision is made. It is important to keep this opening small (2.5 cm to accommodate the single-port device) to minimize air leaks. The single port is placed into the peritoneal cavity with the assistance of a curved clamp, allowing the abdomen to be insufflated with CO2 to a pressure of 12 mmHg. Depending on the manufacturer, the port is set up so that the camera is at the “top” of the triangle; or three 5-mm ports are inserted through the device in a triangular shape, with the camera at the “top” (Fig. 19.2).
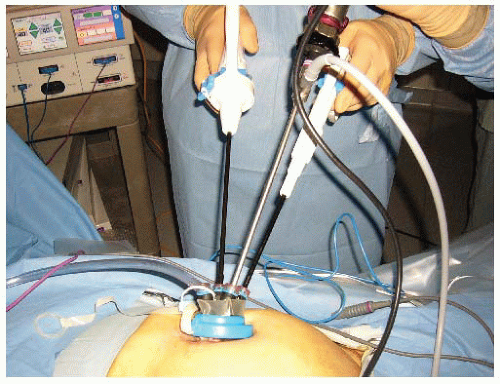 FIGURE 19.2. Insertion of the single port.
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|





