Fig. 3.1
The effect of port length and width on range of movement and triangulation. As the port width (d) is increased, the angle at which instruments meet at the target organ (δ) is increased. This equates to a greater ability to triangulate instruments on the target, a feature of laparoscopic surgery that is often diminished by the SALS approach. Conversely, as the length (L) of the port is increased, the maximum angle at which instruments cross (ϴ) within the port is reduced. This limits the degree of distraction of the instruments possible, thus reducing the range of movement. Therefore the ideal port is a short but wide port that can stretch tissues to avoid the need for a large incision. Of course, if instruments are utilized in a crossed fashion, the requirement for a wide port to allow for triangulation is diminished
SALS access devices also have other special features for consideration. The Storz ports are reusable (although the valves have a limited lifespan and may need replacement). Homemade surgical devices are more affordable. The TriPort+ port has the unique ability to compress the abdominal wall at the access site. This has the effect of reducing the depth and increasing the width of the access site, hence increasing the range of movement and capacity for triangulation, a feature that is particularly useful in obese patients. Another unique feature of the GelPOINT and TriPort+ ports is that the ability to insufflate into a soft-walled channel allows radial force to be applied to the channel, thus maintaining an air lock. The GelPOINT also allows for the insertion of any number of trocars or the surgeon’s choice. The SILS port (Covidien) is a solid port and so results in fewer instrument clashes within the port, affording a greater degree of triangulation.
Access device insertion is unique to each port. For example, with the SILS port, the camera channel (if using a 10 mm laparoscope) needs to be the most inferior channel therefore deflecting the other channels upwards to avoid peritoneal puncture during a TEP inguinal hernia repair. The access strategies for each individual hernia repair will be discussed below.
In summary, the choice of ports needs to suit the surgeon, procedure, and patient. It is hard to be proscriptive. Multiple publications have supported the use of each individual device.
3.2.1.2 Vision
One of the most important decisions the surgeon must make in undertaking SALS is the choice of videolaparoscope, of which multiple designs are available. The size of the laparoscope will be a balance between the reduction in crowding at the access device afforded by the 5 mm laparoscopes and the increased light provided via a 10 mm laparoscope. Furthermore, long and short laparoscopes are available which allow surgeons to try and avoid external clashing with instruments depending on their choice of instrument. Videolaparoscopes can be either rigid rod designs, with 0−45° tips, or flexible tip laparoscopes (e.g., the Storz ENDOCAMELEON® and the Olympus ENDOEYE Flex 3D). Rigid laparoscopes are more familiar for camera operators but offer a more limited view than flexible tip laparoscopes. However, the surgeon must consider the suitability of an angled rod laparoscope or flexible tip laparoscope to each procedure. For instance, in performing TEP inguinal hernia repairs, there is often not enough space to adequately use an angled or flexible tip laparoscope without unduly increasing the dissected space.
Once a laparoscope has been selected, the camera operator must be adequately trained in SALS procedures to provide the correct balance between optimal vision and limited external clash with instruments. Here, the author would like to introduce the concept of “soft but hard” camera operation. In essence, the surgeon will define a set point for the camera operator to fix to, essentially the site of current dissection. If, in the course of performing the required maneuvers at that location, it is necessary for the surgeon to clash with the camera operator, he/she should allow the laparoscope to be deflected away from the set point on application of a certain amount of pressure from the surgeon but then rapidly return to the set point at the end of the maneuver. Familiarity between surgeon and camera operator facilitates this exercise. It is the author’s experience that the challenges of SALS are amplified by novice camera operators. Therefore, establishing a single team for these procedures is essential.
3.2.1.3 Instruments
At the inception of SALS, new instruments were designed to compensate for the loss of triangulation that laparoscopic surgeons had become accustomed to. In general, these included rigid straight instruments, rigid curved instruments, and flexible instruments (which were single-use instruments). Economic considerations now influence the uptake of these instruments in SALS today.
A consideration common to all instruments is the size and shape of the handle, as well as the diathermy connection position. Ideally, a low profile handle will produce less hand clashes. Also, some types of handle ratchets may increase external clash (e.g., Manhes swing-away ratchet, Storz). Olympus has designed their handles to incorporate the diathermy lead connection to minimize external clash (HiQ LS series from Olympus). Rigid curved instruments may have a single curve or a double curve. It may be more appropriate to consider using a combination of straight and curved instruments to suit the procedure.
3.2.2 Technique
In general, the techniques of performing each type of hernia repair using the SALS approach are identical to those performed using multiple port laparoscopic procedures. There are a few general principles of SALS to consider.
1.
The author would like to introduce the concept of instrument shadow (Fig. 3.2a). This concerns the loss of range of movement experienced when two instruments are inserted into a single port. Essentially, if one instrument is fixed in position, the range of movement of the second instrument will be limited by clashes with the fixed instrument. Therefore, changes in the angle between the two instruments will change the regions of inaccessibility by the active instrument – the instrument shadow. This effect alters if a rotating port is used. Furthermore, the instrument shadow will be increased by incremental advancement of the laparoscope (Fig. 3.2b). In a laboratory setting, we have found that a distance of at least 6 cm from the target is required to minimize instrument shadow. The instrument shadow can be further minimized by dynamic use of both instruments.
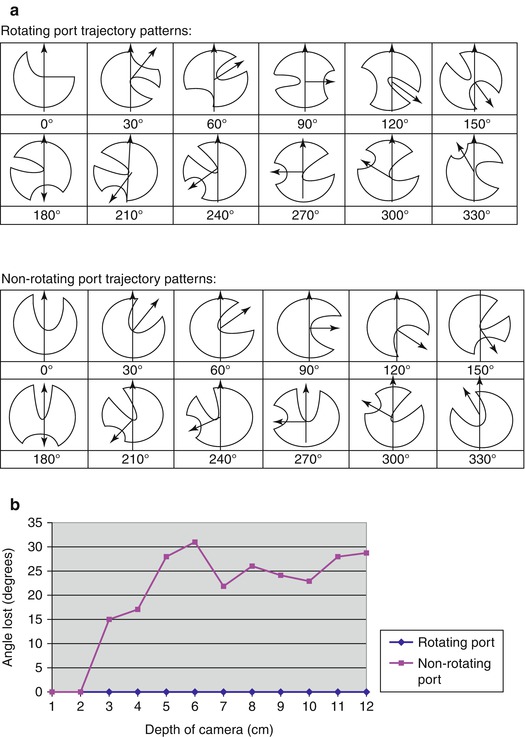
Fig. 3.2
The effect of instrument shadow in SALS procedures. (a) Using a fixed camera position and a fixed instrument, the positions that a second instrument can access is defined with varying angles between fixed instrument and camera. The resulting shadow varies depending not only on the angle but also on whether a rotating or nonrotating port is used. It should be noted that any shadow created using a rotating port is dynamic – that is, the shadow can be rotated to allow access to the “concealed” area without changing the angle of the instruments. (b) The further a laparoscope is advanced into the operative field (and so the closer it is to the objective), the more likely the camera is to behave as a third instrument. This will have the effect of introducing a new instrument shadow, thus reducing the degrees of movement available for the instruments. A minimum distance of 6 cm advancement of the laparoscope through the port is recommended to limit this effect
2.
The author would advocate a “fly-by-wire” operating technique. Many surgeons try to analyze hand movements and maintain uncrossed instruments. A less frustrating strategy would be to accept that instruments will cross and clash. Thus, the objective becomes to minimize the impact of clash but accept the cross. This can best be achieved by avoiding the micromanagement of each component of each maneuver. Rather, one should concentrate instead on the final goal and leave geometric calculations to the “subconscious brain,” in a manner akin to robotics and modern aircraft design.
3.
Many surgeons can perform surgical tasks equally well with both hands. However, if handedness is problematic in SALS (particularly when instruments are crossed), one strategy is to work with one instrument on top of the other. Movements are therefore up and down rather than left and right, making handedness issues redundant.
4.
Get Clinical Tree app for offline access

Strategies to reduce external clashing of handles include pronation of both hands (Fig. 3.3), changing lengths of instruments, or adjusting the assistant position.

Fig. 3.3
 Single-Incision Laparoscopic Appendectomy
Single-Incision Laparoscopic Appendectomy
 Single Access Laparoscopic Cholecystectomy
Single Access Laparoscopic Cholecystectomy
 Single-Access Robotic Surgery
Single-Access Robotic Surgery
 Single-Access Laparoscopic Approach for Pancreatic Surgery
Single-Access Laparoscopic Approach for Pancreatic Surgery
 Single-Access Laparoscopic Right Hemicolectomy
Single-Access Laparoscopic Right Hemicolectomy
 Single-Access Laparoscopic Approach for Gastric Surgery (Hiatal Hernia Repair and Gastric Resections)
Single-Access Laparoscopic Approach for Gastric Surgery (Hiatal Hernia Repair and Gastric Resections)




Demonstration of the pronated hand position during a SALS TEP hernia repair. In this way, even “Manhes swing-away ratchet” can be kept out of the way and handle clashes minimized. This is particularly true if the up/down distraction technique is used. However, if diathermy leads are attached to the top of the instrument, this hand position will bring the lead into play, and consideration for low profile handles is encouraged
Related posts:
Single-Incision Laparoscopic Appendectomy
Single Access Laparoscopic Cholecystectomy
Single-Access Robotic Surgery
Single-Access Laparoscopic Approach for Pancreatic Surgery
Single-Access Laparoscopic Right Hemicolectomy
Single-Access Laparoscopic Approach for Gastric Surgery (Hiatal Hernia Repair and Gastric Resections)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree