Fig. 16.1
Port configuration. C 12 mm camera port. L1 5 mm laparoscopic assistant port. R1 and R2 8 mm robotic working ports for arms 1 and 2 during splenic flexure mobilizations. R1, R3, and R4 8 mm robotic working ports for arms 1, 2, and 3 for sigmoid colon and possible pelvic dissection
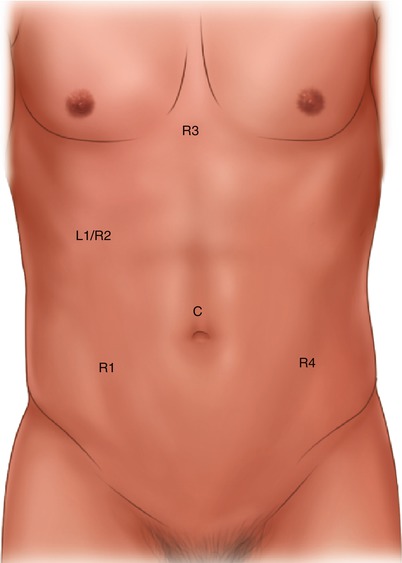
Fig. 16.2
Port configuration. C 12 mm camera port. L1 12 mm assistant port during sigmoid colon and possible pelvic dissections. R1, R2, and R3 8 mm robotic working ports for arms 1, 2, and 3 during splenic flexure and sigmoid colon mobilizations. R1 and R4 8 mm robotic working ports for arms 1 and 2 during limited pelvic dissection
For port configuration 1, a 5 mm trocar as the assistant port L1 is placed in the right flank to help with the splenic flexure mobilization. A total of four 8 mm trocars are placed: one in the right upper quadrant (RUQ), the right lower quadrant (RLQ), left lower quadrant (LLQ) and left flank (see port configuration 1). It is important to follow an “8 cm rule” for port placement as depicted. This helps to standardize the port location, minimizing port variability and avoiding robotic arm collisions. The RUQ port R2 is placed 2 cm below the rib border at the level of the midclavicular line; this will aid in the mobilization of the proximal transverse colon and splenic flexure takedown. The RLQ port R1 is placed 8 cm lateral to the midline at the point of crossing with an imaginary line from the umbilicus to the anterior superior iliac spine. The ports R3 and R4 are reserved for the second part of the procedure, which involves pelvic dissection. The LUQ port R3 is placed 8 cm away from the camera port in a plane 2 cm inferior to the camera port. The left flank port is generally placed at the level of 2 cm superior to the anterior superior iliac spine. It is critical to avoid placing this port too lateral so as to prevent instrument clashing with the iliac bone during mobilization of the distal sigmoid colon and rectum. R1 and R2 are used for the splenic flexure mobilization.
In Fig. 16.2, the robotic port R2, now inserted through a 12 mm assistant port L1, is moved more inferiorly and the robotic port R3 moved toward the midline and superiorly (see Fig. 16.2). Robotic port R4 is mirrored with R1 and needed only if pelvic dissection is necessary.
The most common extraction site is the Pfannenstiel location as described below, but a muscle-splitting LLQ extraction site can be utilized if the final step of the anastomosis is performed under laparoscopic guidance. In this case, the LLQ port would be enlarged to a size to accommodate the extraction of the sigmoid colon through a wound protector.
Operative Steps (Table 16.1)
Table 16.1
Operative steps
Operative steps | Degree of technical difficulty (scale 1–10) |
|---|---|
1. Exploratory laparoscopy and robotic docking | 1 |
2. Mobilization of the descending colon and splenic flexure with identification and ligation of the inferior mesenteric vein | 5 |
3. Identification of the ureter and ligation of the inferior mesenteric artery | 4 |
4. Mobilization of the sigmoid colon | 2 |
5. Transection of the sigmoid colon | 2 |
6. Anastomosis with leak test | 2 |
Here, we describe the robotic specific approaches to the six common steps of a sigmoid resection. As described in the section about the hybrid approach, the mobilization of the splenic flexure can be more challenging than the laparoscopic approach especially in the obese patient. If it is done in a single-docking technique, the medial-to-lateral approach is typically the only option. The lateral approach may be limited to a more time-consuming double-docking technique coming from the left shoulder.
Exploratory Laparoscopy and Robotic Docking
The procedure commences with laparoscopic exploration. At this point, the peritoneal cavity is thoroughly examined and adhesiolysis is performed, if needed. The robotic cart is typically docked on the left side of the patient’s lower extremities in an acute angle. An alternative setup is placing the robotic cart between the legs of the patient. However, this configuration should be avoided if an intracorporeal anastomosis is anticipated, as it would require complete undocking to introduce a circular stapling device. Additionally, one must recognize that with the robotic cart placed between the legs, perineal access is hindered for transrectal or transvaginal specimen extraction. Therefore the left-side cart docking is favored, since it allows enhanced versatility, easier access to the left upper quadrant for full left colon mobilization, and a perineal approach. This configuration affords a safe colorectal anastomosis without undocking the robotic cart with a more reliable robotic-assisted suture repair, if needed.
Mobilization of the Descending Colon and Splenic Flexure with Identification and Ligation of the Inferior Mesenteric Vein
The first segment of the procedure involves mobilization of the descending colon with utilization of the retroperitoneal plane. The first robotic arm is placed in the RLQ port site R1, serves as the surgeon’s dominant hand, and employs a monopolar energy device. The second arm is placed in the RUQ port site R2, serves as the surgeon’s nondominant hand, and uses a bipolar energy device. The third arm is placed in the UM port site R3 and utilizes grasper forceps. The assistant port if available through the left flank port is employed for suction, irrigation, and retraction. During this portion of the procedure, the LLQ port is not used.
The small bowel loops are mobilized out of the operative field superiorly and toward the right. A medial-to-lateral approach for the left colon mobilization is favored to the lateral one due to often times restricted instrument length of the working instrument from the RLQ port to reach around the splenic flexure. This is further limited due to the robotic positioning coming from the left lower side of the patient. This technique allows direct dissection in the avascular retroperitoneal plane. In addition, traction and dissection of the medial retroperitoneal plane is facilitated with the descending colon partially fixed to the abdominal wall by its lateral attachments. This enhanced maneuverability permits prompt identification of critical structures such as the left ureter and vascular pedicles (see Video 16.1).
Related posts:
 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Single-Port Robotic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Robotic Approach
 Operating Room Setup and General Techniques in Minimal Invasive Colorectal Surgery
Operating Room Setup and General Techniques in Minimal Invasive Colorectal Surgery
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach
 Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


