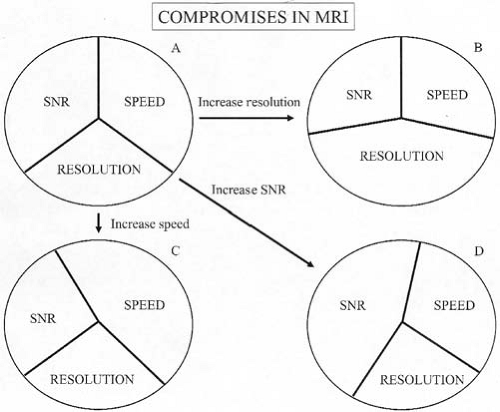
To be successful in magnetic resonance imaging (MRI), one must learn the art of compromise. With few exceptions, when attempting to optimize a scan, a positive change in one sequence parameter exacts a negative price elsewhere. In general, three key elements should be considered when planning and optimizing a scan: signal-to-noise ratio,* scan time, and image resolution. A beneficial change in one of these three elements usually results in an undesirable change in at least one of the other two elements (Figs. 1.20, 1.21).
FIG. 1.20. Compromises in MRI. Any pulse sequence begins with potential signal-to-noise ratio (SNR), resolution, and scan time (speed) (A). Improvements in any of these three parameters results in decrement in one or both of other two parameters (B, C, D).
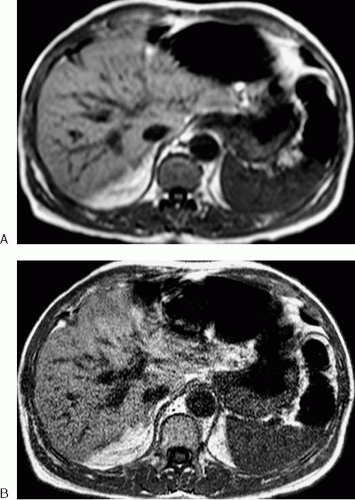
FIG. 1.21. Compromises in MRI. A: T1-weighted gradient echo image optimized for signal-to-noise ratio and time (10-second scan time) by using thick slices (10 mm) and fewer phase-encoding steps (112 × 256 matrix). Minimal background noise is present, but resolution is relatively poor and edges are blurred. B: Image optimized for resolution (246 × 512 matrix, 5-mm slice thickness) demonstrates considerably more noise and required 36-second scan time for same coverage.
Often, the MR clinician can control which elements to compromise when optimizing one particular aspect of a scan. For example, improvements in the signal-to-noise ratio can be attained by increasing the number of signal averages (which increases scan time) or by reducing the image matrix (which decreases resolution). Similarly, one can perform a quicker scan by reducing the number of phase-encoding steps (decreasing resolution) or by reducing the number of signal averages (decreasing the signal-to-noise ratio). In addition to these compromises, some attempts at image optimization result in artifacts. For example, switching from a breath-hold sequence to a non-breath-hold sequence to improve the signal-to-noise ratio not only increases scan time, but motion-related artifacts increase if additional steps are not taken to prevent them.
In this section, strategies to reduce acquisition time, improve spatial resolution, increase the signal-to-noise ratio, and reduce common artifacts in abdominal and pelvic MRI are discussed. Although most strategies require some form of compromise, there are new techniques that accomplish these improvements with minimal discernible penalty. However, the capacity to employ these latter techniques must be purchased from the manufacturer, often at considerable expense, resulting in a different form of compromise.
Reducing Scan Time (Improving Temporal Resolution)
One impediment to the success of abdominal and pelvic MRI has been the amount of time it takes to complete a study. At many institutions, appointment times of 1 hour or more are typical for even the most basic abdominal MRI protocols. As a result, many MR practices do not solicit abdominal and pelvic examinations. The benefits of reduced scan time, however, go beyond patient throughput. Quicker scans result in fewer artifacts from physiologic motion and reduced patient fatigue.
There are three primary approaches to shortening scan time. The first involves modifying the basic acquisition parameters for an existing sequence. This strategy is only effective to a limited extent, because modifying some parameters beyond certain limits results in undesirable changes in image contrast, resolution, or quality. The second strategy requires the use of a different sequence (e.g., substituting a gradient echo for a spin echo T1-weighted sequence). The success of the sequence-substitution approach depends on such factors as magnetic field strength, gradient strength, and available software. The third approach involves innovative shortcuts, most of which entail undersampling k-space and require special software or hardware. To optimize efficiency, more than one of the time-saving methods may be used in combination. However, one should not spend more time optimizing the sequence than it would take to complete the original sequence.
Parameter Modifications
Table 1.2 summarizes the parameter modifications most commonly used for reducing scan time. For a conventional spin echo or gradient echo sequence, acquisition time is given by the following equation:
Imaging time = (repetition time [TR]) (number of phase-encoding steps) (number of signal averages)
TABLE 1.2. Parameter modifications to reduce scan time
Increased image blurring; increased magnetization transfer effects
FOV, field of view; SNR, signal-to-noise ratio; TR, repetition time.
According to the above equation, steps that reduce the TR, number of phase-encoding steps, or number of signal averages will save time. MR technologists routinely vary the TR to reduce scan times. However, decreasing the TR beyond a certain point for a multislice acquisition actually increases scan time, because fewer slices can be acquired during the shorter TR. The rectangular field-of-view option saves time, because it allows fewer phase-encoding steps to be performed along one axis (usually anteroposterior for abdominal and pelvic examinations).
Other factors also play a role in acquisition time. The sampling bandwidth refers to the rate at which the echo is digitally sampled. More rapid sampling reduces acquisition time (and reduces chemical shift artifact) but increases image noise. Long echo train lengths reduce the number of excitations required to make an image. With sufficiently long echo train lengths, breath-hold T2-weighted imaging of the abdomen is possible. However, image blurring and magnetization transfer effects (which can affect solid lesion conspicuity) may become clinically significant with long echo train lengths. For this reason, the echo train length is generally kept below 16.
A more complete list of the various effects caused by changing MRI parameters is found in Section 4.3.
Sequence Substitutions
Table 1.3 demonstrates time-saving sequence substitutions. Extensive clinical experience suggests that T1-weighted spoiled gradient echo and T2-weighted fast spin echo can be routinely substituted for conventional spin echo sequences for most abdominal applications. Experience with single-shot (e.g., HASTE), gradient and spin echo hybrid (e.g., GRASE), and magnetization-prepared (e.g., MP-RAGE) techniques is considerably less. Therefore, these sequences are often used to supplement more traditional sequences or are reserved for uncooperative patients. These latter sequences are also continuously being improved by vendors. As a result, a scanner with state-of-the-art gradients and the most recent software release is more likely to yield clinically acceptable results with newer rapid imaging techniques than an older scanner. To determine the appropriateness of a particular sequence substitution in a particular practice, we recommend performing both the sequence to be replaced and the substitution under consideration until it is clear that important diagnostic information is not being lost.
TABLE 1.3. Sequence substitutions to reduce scan time
Substitution
Tradeoff
Gradient echo T1 for spin echo T1
Reduced SNR; increased susceptibility artifact
Fast spin echo for spin echo
Brighter fat may necessitate use of fat suppression
Single shot for multishot
Reduced SNR; loss of image sharpness; reduced conspicuity of solid lesions
GRASE for spin echo type sequences
Limited clinical experience
Magnetization prepared gradient echo for spoiled gradient echo (see MP-RAGE)
Limited clinical experience
GRASE, gradient and spin echo hybrid; SNR, signal-to-noise ratio.
Additional Techniques for Reducing Scan Times
Half-Fourier (1/2 NEX, Half Scan)
During MR data acquisition, the phase-encoding gradient is applied in equal increments on either side of the zero phase-encoding step. As a result, k-space is symmetric in the phase-encoding direction. It is therefore possible to create a clinically useful image from a fraction of k-space (slightly more than half). This technique is commonly applied with single shot acquisitions commonly referred to as HASTE, ssTSE, or ssFSE. Figures 1.41 and 1.43A are examples of HASTE images.
Partial or Fractional Echo Sampling
K-space is also symmetric in the frequency-encoding direction. Therefore, one can sample roughly half of each echo during application of the frequency-encoding gradient. This technique allows for a shorter minimum TE.
Zerofill Interpolation (ZIP, Reduced Acquisition)
Like the preceding techniques, zerofill interpolation involves collecting only a portion of the data necessary to fill k-space. In a common variation of this technique, the central lines of k-space are collected and the remaining peripheral portions of k-space are filled with zeros to allow a Fourier transform to be performed. Three-dimensional (3D) MR angiography (MRA) and gradient echo sequences used for dynamic contrast-enhanced imaging of the liver, pancreas, and kidneys often employ zero-fill interpolation. In this manner, high-resolution breath-hold imaging of the abdomen can be performed. Truncation artifacts are exacerbated with zero-filling, but this is rarely of clinical importance at the matrix sizes typically used. Fast 3D gradient echo imaging combined with zerofill interpolation is commonly referred to as VIBE (volumetric interpolated breath-hold examination). Many of the contrast-enhanced 3D gradient echo images found throughout this text were performed with zerofill interpolation.
Keyhole
Keyhole imaging is primarily applicable to dynamic contrast-enhanced scanning of a limited number of slices. Instead of filling only a portion of k-space for each image, the keyhole technique involves collecting a full set of image data at the beginning of the examination including both the high spatial resolution portions of k-space and the low spatial resolution portions responsible for image contrast. After the administration of an intravenous bolus of contrast material, subsequent acquisitions acquire only the central (high image contrast) portions of k-space. The peripheral, high spatial resolution portions of k-space are filled using data from the initial reference image. This dramatically reduces overall scan time, allowing for rapid dynamic contrast-enhanced imaging.
Only gold members can continue reading. Log In or Register to continue
 Basic Magnetic Resonance Imaging Principles for the Abdomen and Pelvis
Basic Magnetic Resonance Imaging Principles for the Abdomen and Pelvis
 Magnetic Resonance Urography
Magnetic Resonance Urography
 Magnetic Resonance Imaging of the Gastrointestinal Tract
Magnetic Resonance Imaging of the Gastrointestinal Tract
 Modifying Sequence Parameters
Modifying Sequence Parameters
 Glossary of Magnetic Resonance Imaging Terms
Glossary of Magnetic Resonance Imaging Terms
 What the Surgeon Needs to Know: Preoperative Assessment of Patients with Selected Tumors and Organ Transplant Candidates
What the Surgeon Needs to Know: Preoperative Assessment of Patients with Selected Tumors and Organ Transplant Candidates



