Robotic Single-Port Right Hemicolectomy
Vincent Obias
Sherif Selim
KEY STEPS
1. Insertion of ports: gelpoint placed through 4-cm incision through umbilicus.
2. Patient rotated to the left and slightly Trendelenburg.
3. Laparoscopic assessment and then small bowel and omentum moved toward left upper quadrant.
4. Robot will be docked replacing the laparoscope.
5. Ileocolic pedicle defined and divided, protecting the ureter and the duodenum.
6. Division of the right branch of the middle colic.
7. Full medial-to-lateral mobilization of the cecum, ascending colon, and hepatic flexure.
8. Hepatic flexure mobilization completed using a superior approach.
9. Cecum retracted cranially and laterally to complete mobilization of the cecum and small bowel mesentery off the retroperitoneum.
10. Confirmation of full mobilization of the right colon to midline.
11. Extension of umbilical port site and exteriorization of the right colon.
12. Standard extracorporeal resection and anastomosis.
ADDITIONAL ADVICE
1. When dissecting, one limitation may be the camera preventing arms no. 1 and no. 2 from dissecting or grasping a certain area. Moving the camera away from the area in question and dissecting or grasping this area in the peripheral portion of the surgeons view may help.
2. The gelport has a built in wound protector for cases associated with cancer.
PATIENT POSITIONING
The patient is placed supine on the operating room (OR) table on a bean bag. After induction of general anesthesia and insertion of an oral gastric tube and Foley catheter, the legs are placed in yellow fin stirrups. The arms are tucked at the patient’s side and the bean bag is aspirated. For more obese patients who will not fit on the OR table, the left arm is left out from the side. The abdomen is prepared with antiseptic solution and draped routinely.
INSTRUMENT POSITIONING
The primary monitor is placed on the right side of the patient at about the level of the shoulder. The secondary monitor is placed on the left side of the patient at the same level and is primarily for the assistant or observers. The operating nurse’s instrument table is placed to the right of the patient’s legs. The assistant is on the left side of the patient. A 30-degree camera lens is preferred.
UMBILICAL PORT INSERTION
A 4-cm vertical incision is made through the umbilicus. This is deepened down to the linea alba, which is then grasped on each side of the midline using Kocher clamps. Cautery is used to open the fascia between the Kocher clamps and Kelly forceps are used to open the peritoneum bluntly. Having confirmed entry into the peritoneal cavity, the gelport is inserted. A 12-mm port and three 5-mm laparoscopic ports are inserted into the gelport. Two of the 5-mm ports will be removed at the time of the switch to the robotic ports.
SINGLE-PORT ROBOTIC SETUP
The assistant now moves to the patient’s left side, standing caudad to the surgeon. The patient is rotated with the right side up and left side down, to approximately 15 to 20 degrees tilt, and often as far as the table can go. This helps to move the small bowel over to the left side of the abdomen. The patient is then placed in a slightly Trendelenburg position. This again helps gravitational migration of the small bowel away from the operative field. The surgeon then inserts two atraumatic bowel clamps. The greater omentum is reflected over the transverse colon so that it comes to lie on the stomach (Fig. 14.1). If there is no space in the upper part of the abdomen, one must confirm that the orogastric tube is adequately decompressing the stomach of gas. The small bowel is moved to the patient’s left side, some remaining in the pelvis and upper abdomen, allowing visualization of the ileocolic pedicle.
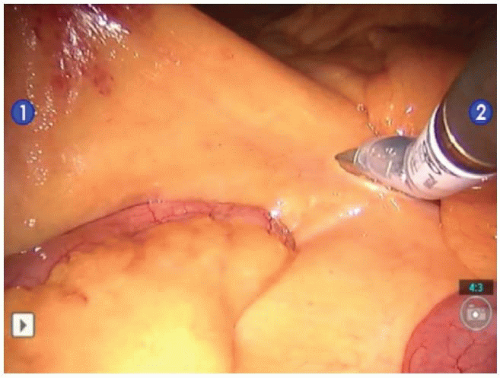 FIGURE 14.1. The greater omentum is reflected over the stomach to make space and facilitate visualization of the ileocolic pedicle. |
ROBOTIC SINGLE-PORT DOCKING
Dock robot to the right side of patient, perpendicular to patient.
Cross robotic arms no. 1 and no. 2 at fascia.
Use 30 degree up scope which goes below the two arms.
Can use a 5-mm assistant port through gelport.
The robotic arms are switched on the console manually so the surgeon controls what he/she views as the correct instrument internally.
The robot comes from the right side of the patient at a perpendicular angle. Two 8.5-mm robotic ports are placed through the gelpoint for the two robotic arms. Arms no. 1 and no. 2 are crossed at the level of fascia (Figs. 14.2 and 14.3). The left arm of the robot crosses and becomes the right instrument inside and vice versa. A 30-degree scope in the up position is used which is placed below the two arms. One 5-mm port is left to be used by the assistant. Robotic arms no. 1 and no. 2 are switched manually on the robotic console so the surgeon controls what he/she views as the correct instrument internally.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


