Fig. 9.1
Port configuration. C 12 mm camera port, L1 optional 5 mm assistant port, R1 and R2 8 mm working ports for arm 1 and 2, R3 optional 8 mm working port for arm 3
An additional 8 mm port (R3) can be placed in the right lower quadrant (RLQ). This would enable docking of the third robotic arm to use an additional fenestrated grasper for retraction. Typically, a 30-degree camera, robotic hook cautery, or endoshears on the left robotic arm (R1) and a bipolar fenestrated grasper on the right robotic arm (R2) are employed.
Extracorporeal anastomosis is most commonly performed and therefore the extraction site is typically above the umbilicus by extending the 12 mm camera port superiorly. If the 12 mm camera port is located left lateral to the umbilicus, this can also be enlarged to a transverse incision for extraction.
Operative Steps (Table 9.1)
Table 9.1
Operative steps
Operative steps | Degree of technical difficulty (scale 1–10) |
|---|---|
1. Exploratory laparoscopy and docking | 2 |
2. Identification an ligation of the ileocolic vessels | 3 (medial to lateral) |
3 (lateral to medial) | |
3. Dissection of retroperitoneal plane and identification of the duodenum | 3 (medial to lateral) |
3 (lateral to medial) | |
4. Mobilization of the right colon and terminal ileum | 2 |
5. Mobilization of the proximal transverse colon and hepatic flexure | 4 |
6. Identification and ligation of the middle colic vessels | 6 |
7. Extracorporeal anastomosis, (alternative) closure and reinspection | 2 |
Intracorporeal anastomosis | 3 |
The steps of a robotic right hemicolectomy are similar to the laparoscopic approach. Depending on the availability of robotic equipment, a various degree of steps are preformed robotically and some laparoscopically, hence resulting in a hybrid procedure. A total robotic approach includes robotic ligation of vascular pedicles, bowel transection, and intracorporeal anastomosis, which will be described in more detail in a separate chapter.
Exploratory Laparoscopy and Docking
Pneumoperitoneum is established through the Veress needle in the LUQ or above the umbilicus and subsequent direct insertion of the 12 mm port or using Optiview technique in the periumbilical location. The 12 mm port can be placed also through the Hasson technique. It is important to use a bariatric length trocar to allow enough space for attaching the robotic arm. The two 8 mm robotic ports and the 5 mm assistant ports are inserted under direct vision. Diagnostic laparoscopy is performed. Following port placements, the patient is placed in the Trendelenburg position (15–20°) with a left tilt; sometimes no Trendelenburg is helpful if small bowel loops can be left in the pelvis. The terminal ileum and the ascending colon are exposed; the remainder of the small bowel is placed towards the left upper quadrant of the abdomen or the pelvis.
The robot is typically docked from the right side of the patient. The robotic field of dissection is typically less than 180° wide. Therefore, small bowel loops may have to be lysed if adhesed to the pelvis first laparoscopically. Similarly, if dissection needs to be extended towards the mid transverse colon, the robot can be docked more from the right upper quadrant. The surgical assistant is on the left of the patient.
Identification and Ligation of the Ileocolic Vessels
The cecum is held and tented up through port R2 and the ileocolic pedicle dissected at the base and isolated through R1 (see Fig. 9.2). The assistant via the 5 mm port uses an energy device to transect the ileocolic pedicle at the origin (see Video 9.1). The other possibility is to use a robotic energy sealer, which is exchanged for the monopolar instrument in R1 (see Video 9.2). Alternatively, both artery and vein can be dissected out and ligated using hemoclips through R1. Extracorporeal vascular control of the ileocolic pedicle can be undertaken after the lateral to medial approach in benign cases.
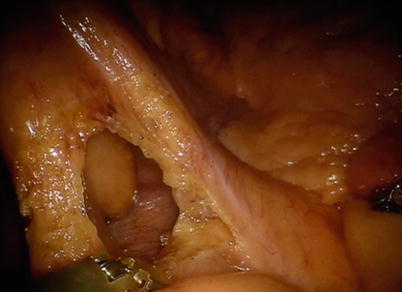
Fig. 9.2
Isolation of ileocolic pedicle
Dissection of the Retroperitoneal Plane and Identification of the Duodenum
The dissection of the retroperitoneal structure is continued as far from medially as possible after identification of the duodenum (see Fig. 9.3). The assistant tents up the ascending colon mesentery through the laparoscopic port L1.
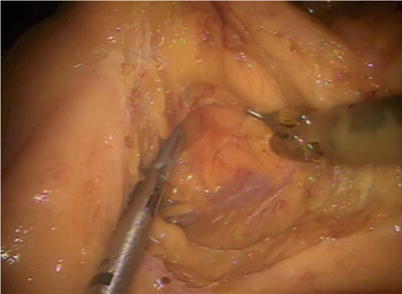
Fig. 9.3
Medial to lateral dissection
Mobilization of the Right Colon and Terminal Ileum
The cecum and the ascending colon are grasped both by the fenestrated grasper in R2 as well as the assistant, retracted medially and superiorly and the dissection started along the white line of Toldt in the right paracolic gutter (see Video 9.3). If a fenestrated grasper in R3 is used through the RLQ port, it can facilitate retraction, by either pushing the cecum or ascending colon medially or lifting the peritoneum lateral to the line of Toldt. The dissection is carried out in the avascular plane from the cecum to the hepatic flexure with continuous gentle traction medially. Care should be taken to identify and to stay anterior to the second part of the duodenum if not identified previously. Identifying the anterior aspect of the second part of duodenum in the lateral approach denotes sufficient mobilization of the right colon and the mesentery with the pedicle (see Fig. 9.4).
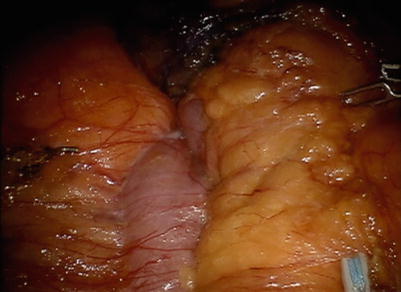
Fig. 9.4
Lateral to medial dissection
Mobilization of the Proximal Transverse Colon and Hepatic Flexure
Facilitation of this might need undocking the robot and changing the patient position to a reverse Trendelenburg position with left tilt. Hook diathermy or endoshears are now used through R2 and a fenestrated grasper in R1. The gastrocolic omentum is taken down to enter the lesser sac (see Fig. 9.5 and Video 9.4). R1 retracts the transverse colon caudally while R2 dissects the omentum off the colon wall. The assistant helps with retracting the transverse colon while R3 (if used) can provide countertraction by retracting omentum or the gallbladder cephalad. The hepatocolic ligament is taken down similarly, and complete mobilization of proximal transverse colon and the hepatic flexure is accomplished. The hepatic flexure also can be taken down from the lateral to medial approach (see Fig. 9.6 and Video 9.5).
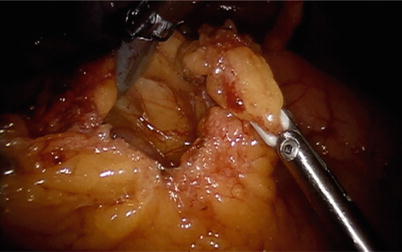
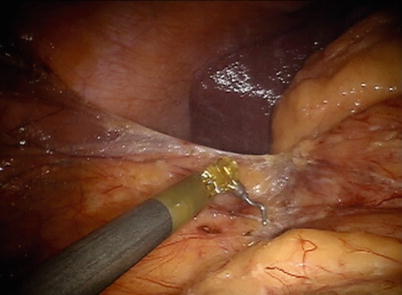
Fig. 9.5
Entry into lesser sac
Fig. 9.6
Hepatic flexure mobilization
Identification and Ligation of the Middle Colic Vessels
The right branch of the middle colic vessels can be similarly ligated by either using the assistant’s 5 mm port or using a robotic vessel sealer through R2. The approach is similar to the supramesocolic approach described in previous chapters.
Related posts:
 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Single-Port Robotic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Robotic Approach
 Operating Room Setup and General Techniques in Minimal Invasive Colorectal Surgery
Operating Room Setup and General Techniques in Minimal Invasive Colorectal Surgery
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach
 Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


