Fig. 10.1
Operating room setup. With permission from Gossedge G, Jayne D. Robotic Technique for Right Colectomy. In: Kim J, Garcia–Aguilar J, eds. Surgery for Cancers of the Gastrointestinal Tract: A Step by Step Approach. Springer, New York 2015; pp. 187–194
10.3 Positioning, Port Placement, and Docking
10.3.1 Patient Positioning
After intubation and placement of a urinary catheter, orogastric tube, and IV access, the patient is positioned supine with the iliac crest centered over the flexion point joint (break) of the table. The patient’s arms are tucked alongside the body and padded to lessen the possibility of brachial plexus injury. This also allows for easier docking of the robot and provides extra space for the assistant at bedside. Pressure points and bony prominences are padded, and the body is secured to the operating table with straps around the legs and shoulders. We also prefer to use antiskid foam cushion in order to avoid the patient sliding with changes in position. Finally, the patient is covered with an upper body warmer to prevent hypothermia. Sequential compression devices are applied to the legs for DVT prophylaxis. (If needed, the table can be flexed 10–15° at the break to lower the patient’s legs, in order to prevent external collisions with the robotic arms after docking.) Final table adjustments should be made prior to draping, and an initial safety check performed with the bed rotated in all necessary planes—most importantly in Trendelenburg and left-sided tilt position.
10.3.2 Port Placement
When performing robotic-assisted right hemicolectomy, thought must be given prior to port placement and decisions made based upon the patient’s size and body habitus, extent of the dissection of the transverse colon, and whether an intra- or extracorporeal anastomosis is planned. In general, we recommend a 4-trocar approach (camera, two robotic trocars, and an auxiliary laparoscopic trocar) when an extracorporeal anastomosis is planned. In this case, the specimen is extracted by extending the incision used for the camera trocar. The intracorporeal anastomosis requires one additional robotic or laparoscopic large-bore trocar (12–15 mm) to introduce the stapler. Basic principles for port placement dictate that the camera port be 15–18 cm from the site of dissection, and the distance between ports, following insufflation, should be around 8 cm to prevent collisions.
10.3.2.1 Camera Port, 12 mm
Pneumoperitoneum is established either with a Veress needle placed in Palmer’s point so as to achieve insufflation of 12–15 mmHg. A 10–12-mm balloon port for the camera is placed either supraumbilically or to the left of the umbilicus, 2–3 cm medial to the midclavicular line (MCL), depending upon body habitus and site of the lesion. (The spino-umbilical line is drawn from the anterior superior iliac spine to the umbilicus.) Alternatively, the open Hasson technique can be used. The camera is then introduced, and inspection for metastatic disease is performed.
10.3.2.2 Four-Port Robotic Right Hemicolectomy with Planned Extracorporeal Anastomosis
The position of the robotic and laparoscopic trocars is only decided after pneumoperitoneum has been created:
Instrument Arm 1, Vented Robotic Port, 8 mm: Place the port approximately two fingerbreadths below the left costal margin along the left MCL. The distance to the camera port should be at least 8–10 cm. This port should be vented to connect the smoke evacuator.
Instrument Arm 2, Robotic Port, 8 mm: This port is placed in the vicinity of the intersection of the left MCL with the SUL and always more than two fingerbreadths medial to left anterior superior iliac spine. However, it is important to take into consideration the fact that the instrument introduced through this trocar should reach the hepatic flexure and may need to be moved medially in large patients. The distance to other instrument ports and the camera port should be at least 8–10 cm.
Assistant Port (5 mm): Place a 5-mm laparoscopic port lateral to the left MCL, at least 8–10 cm away from both instrument arms.
Instrument Arm 3: Some surgeons prefer to use the third robotic arm to obtain additional exposure during the dissection. An 8- or 12-mm port is placed in the suprapubic area at least two fingerbreadths above the pubic bone.
10.3.2.3 Five-Port Robotic Right Hemicolectomy with Intracorporeal Anastomosis (Fig. 10.1)
When an intracorporeal anastomosis is planned, some surgeons prefer to place the camera port to the left of the umbilicus and at least 2–3 fingerbreadths from the MCL.
Instrument Arm 1 and 2 ports and a laparoscopic auxiliary port are placed for an extracorporeal anastomosis.
For Instrument Arm 3, a 12-mm trocar (either robotic or laparoscopic, depending on the stapling device used) is placed in the suprapubic area, 2–3 fingerbreadths above the pubic bone and to the right of the midline. The incision for this trocar should be in transverse orientation, so that it can be enlarged to create a small Pfannenstiel incision in order to remove the specimen.
10.3.2.4 Exposing the Area of Dissection
Prior to docking the robot, the bed is tilted left side down with slight Trendelenburg positioning. When an intracorporeal anastomosis is planned, the operating room table can be flexed slightly at the hips (kidney bend) to gain additional range of motion for instrument arm 3 and avoid collision with the patient’s legs. After inspecting the peritoneal cavity, the omentum and the transverse colon are pushed cephalad over the stomach using laparoscopic instruments. The small intestine is gently moved to the left to expose the ileocolic pedicle and duodenum.
10.3.3 Robotic Cart Docking and Instrument Placement
A clear path for the patient cart free of all cords and other equipment should be made prior to driving the draped patient cart. The cart should approach the OR table from the right, at a 45° degree angle over the right shoulder.
When docking the arms, it is important to ensure that the camera port, target anatomy, and robotic cart center column are aligned. Port and arm clutch maneuvers should be used to dock the remaining instrument arms. Once the cart is docked, the position of the bed cannot be changed without undocking. While docking, the camera arm should be in the “sweet spot” to maximize range of motion for the camera and instrument arms. The blue arrow should align with the blue marker on the second joint or create a 90° angle between the first and third joint on the camera arm. When using all three instrument arms, it is useful to place the arm joints as lateral as possible away from the field, to avoid collision.
10.3.3.1 Loading the Robotic Arms with Instruments
Four-Port Robotic Right Hemicolectomy with Extracorporeal Anastomosis (Fig. 10.2)
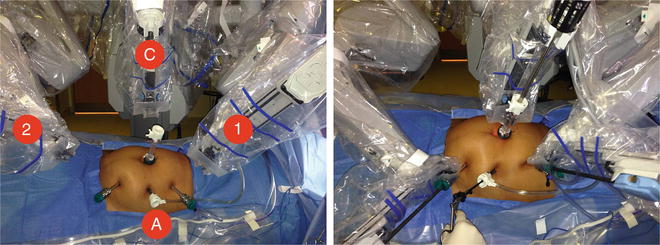
Fig. 10.2




Robotic docking and instrument position
Related posts:





Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
