(1)
Department of Vascular Surgery, Evangelisches Krankenhaus Königin Elisabeth Herzberge, Berlin, Germany
In this chapter we discuss puncture sites, puncture techniques, how to remove cannulas, and the hemodynamic results of single-needle and double-needle dialysis. For a start we will look at morphological changes of the vessel wall after puncture.
17.1 Pathophysiology of the Punctured Vessel Wall
The walls of a vein and of a prosthesis are quite different.
17.1.1 Vein
From a biomechanical point of view, the essential structure of the venous wall is the tunica media, which mainly consists of elastic and muscle fibers. The fibers follow a spiral course with only a slight rise. They cross in a grid pattern. A puncture severs this pattern. At the puncture site, a circumscribed dilation of the wall occurs (Fig. 17.1). Thus narrow venous segments can be dilated intentionally by selective puncturing (Krönung 1984a, b). Apart from the severance of the fibers, the mechanically less resistant connective tissue, which fills the defect, is responsible for the dilation. Frequent punctures of a vein at a specific site will almost always lead to its aneurysmatic dilatation (Fig. 17.2).
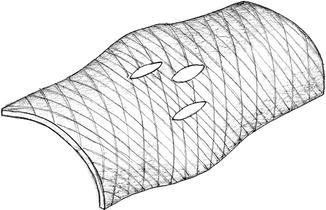

Fig. 17.1
Dilation of the venous wall caused by destruction of the wall structure
Fig. 17.2
Venous aneurysm of a frequently punctured venous segment
17.1.2 ePTFE Prosthesis
The wall of an ePTFE prosthesis shows a nodulous fibrillary structure. Each puncture leaves a wall defect through which connective tissue proliferates into the lumen (Fig. 17.3). Frequent punctures close to each other may then cause stenoses of the prosthesis. Only extensive destruction of the wall structure may lead to aneurysms due to the reduced resistance of the scar tissue.
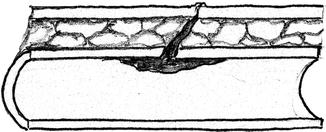
Fig. 17.3
Sprouting of connective tissue through a puncture site into the lumen of an ePTFE prosthesis
17.2 Puncture Site Selection
Basically there are three patterns of how puncture sites are distributed:
Rope ladder puncture
Area puncture
Buttonhole puncture
The choice of puncture sites and their distribution should avoid unfavorable damage to the vessel.
The available puncturable surface of the vessel wall decisively determines the puncture pattern.
17.2.1 Rope Ladder Puncture
Principle
Regular systematic distribution of punctures all over the suitable vessel wall.
Indication
Long(ish) puncturable stretch. For the reasons mentioned above (Fig. 17.1) puncture sites should vary as much as possible as far as topography and time intervals are concerned. Thus the area used for punctures should include large portions of the total surface area of the AV vessel that may be used for punctures (Fig. 17.4).
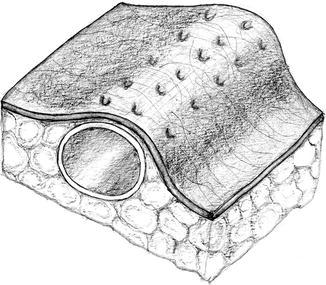
Fig. 17.4
Recommended puncture sites using the whole suited surface
These punctures should follow an individual pattern (e.g., Fig. 17.5).
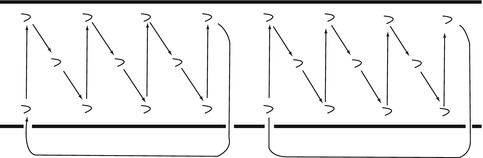
Fig. 17.5
Example for a puncture pattern
17.2.2 Area Puncture
Principle
Even distribution of punctures across a limited area.
Indication
Exclusive indications are:
Only short puncturable segment
Stenosed segment of an AV fistula
Intentional repetitive punctures of a stenosed segment may cause its dilation to allow for its future easier use. Area punctures very often lead to the dilation of the punctured segment.
17.2.3 Buttonhole Puncture
Principle
Punctures of always the exact same site. There are two distinct forms of buttonhole punctures.
Punctures of the Same Site Not Using a Long Subcutaneous Tunnel
We disapprove of this technique for theoretical and practical reasons.
Repetitive punctures of the exact same puncture canal without a long subcutaneous tunnel:
Preclude the occlusion of the canal by connective tissue
Widen the puncture canal (filled with thrombi and closed with slough) with each following puncture
Eventually often lead to a localized inflammation and its possible progression up to a spontaneous perforation (Fig. 17.6a)
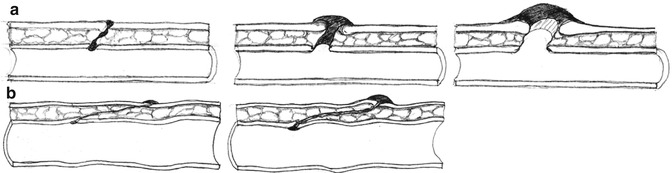
Fig. 17.6
(a) Increasing damage to the puncture site after multiple puncturing. (b) Buttonhole punctures. Creation of a long subcutaneous tunnel by repeated puncturing
Indication
In our opinion this technique is only justified under exceptional circumstances. Instead we recommend the speedy creation of a new vascular access if need be.
Punctures of the Same Site Using a Long Subcutaneous Tunnel
Under special circumstances the conscious systematic puncturing of the exact same site with a long subcutaneous tunnel is chosen.
Principle
Creation of a single subcutaneous tunnel by repeated punctures with sharp cannulas over a 3–4-week period (Fig. 17.6b).
Following a routine with:
(a)
Sufficiently long time for disinfection of the puncture site (several minutes).
(b)
Removal of scab with sterile instruments and repeat long disinfection.
(c)
Puncture vessel via the formed track using a (less sharp) blunt cannula.
Indication
Only limited cannulation sites of an AV fistula with sufficient subcutaneous cover.
Contraindication
Alloplastic material (prosthetic AV shunts).
Requirement
Specially trained and motivated staff.
Evaluation
No personal experience. Plausible good results in specialized centers.
17.3 Puncture Technique
Four factors characterize puncture techniques:
The angle of insertion, which also determines the length of the subcutaneous tunnel
The position of the cannula’s aperture
The way a cannula is inserted into the vessel
The direction of puncture in relation to the flow direction
17.3.1 Angle of Insertion
In order to prevent infections, and for better hemostasis, we recommend a subcutaneous tunnel which is as long as possible. Therefore the angle of insertion should be as acute as possible. For this purpose the cannula needs to be sufficiently long (usual available lengths 5–25 mm with 5-mm intervals). The sketch in Fig. 17.7, which was drawn to scale, shows that only an adequately long cannula can create a long subcutaneous tunnel. The internal resistance of a long cannula is higher, though.










