(1)
Gastroenterology and hepatology, Chinese PLA General Hospital, Beijing, China, People’s Republic
Abstract
Process of tunnel technique for lesions from mucosa, muscularis propria are discussed first and then the anatomic marks within the tunnel. It is often argued that it is difficult to keep orientation and distinguish the mucosal layer from the muscularis propria layer during establishment of a submucosal tunnel, the reason might be that the submucosal tunnel is an artificial cavity and its anatomy is not well understood. In this chapter the anatomic marks to be discussed are those being commonly used when performing tunnel technique nowadays and surely would be more well understood in the future with the development of tunnel technique. The morphology within the tunnel is actually similar to that within the lumen of the esophagus and the cardia. Anatomic marks described in this chapter include the morphology of vessels, the location of vessels, the morphology of the tunnel cavity and the characteristics of the muscle layer.
5.1 Process of Tunnel Establishment
5.1.1 Preoperative Preparation
During the process of tunnel establishment, the patient is under general anesthesia with tracheal intubation and position of the patient is selected as previously discussed (Sect. 4.1). Before anesthesia, endoscopy is routinely performed to ensure that no residues of foods are in the esophagus or the stomach.
5.1.2 Equipments
Endoscopes: Endoscopes with water delivery system are generally used, e.g., Olympus Q 260J, Fuji endoscopy (EG-450RD5) and Pentax endoscopy. If no water delivery system is available, endoscopic electrosurgical knife with water delivery function is recommended.
Gas: CO2 is routinely used during the operation.
High frequency electricity generators: ERBE equipment is a common type for the operation, while ESG-100 from Olympus is also a good choice. The parameters of the equipment are often set according to the output power and the preference of the endoscopists (Detailed in Chap. 11).
Accessories: Injection needle, various endoscopic electrosurgical knives, hemostatic forceps and hemostatic clips.
Solutions for submucosal injection: Commonly used solutions include saline water + adrenalin + Methylthioninium chloride, or Glycerol + Fructose + Methylthioninium chloride, or only saline water, or only Glycerol + Fructose. As for adrenalin, 1 mg is added for each 250 ml solution; and for Methylthioninium chloride, 0.1–0.4 ml is added to each 250 ml of the solution based on personal experience. Compared to saline water, Glycerol + Fructose solution may cause smoke during electrocoagulation and obscure the operational vision, but it has a longer submucosal duration time compared to saline water.
5.1.3 Procedure of Tunnel Technique
Determine site of incision: Choose an appropriate target site for entry incision based on the locations and types of the lesions.
Submucosal injection: 23–25 G injection needle or Hybrid knife could be used for submucosal injection to lift the local tissue.
Incision: Transverse or longitudinal incision could be used, with an incision length around 1.2 cm (Fig. 5.1a) for a transverse incision and 1.5–1.8 cm (Fig. 5.1b) for a longitudinal incision.
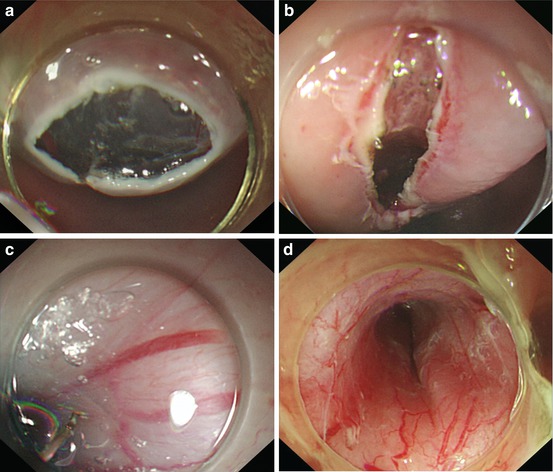
Fig. 5.1
(a) Transverse entry incision. (b) Longitudinal entry incision. (c) Tunnel establishment with a depth of SM2-SM3. (d) Tunnel established with a width of 1.5–1.8 cm
Submucosal dissection: After incision, the submucosal injection is performed in the front part of the incision, and then the mucosal layer is little by little dissected from the muscularis propria with a depth of SM2-SM3 (Fig. 5.1c). The dissection is gradually performed forward along the muscularis propria to make room for the transparent-cap attached endoscope to be maneuvered between the mucosa and muscularis propria.
Tunnel establishment: With repeated injections, the mucosa and muscularis propria are dissected for a length enough to establish a tunnel with a width of 1.5–1.8 cm (Fig. 5.1d).
Treatment: After completion of establishment of a submucosal tunnel, treatments are performed on lesions of mucosal layer, esophageal achalasia and SMTs from muscularis propria.
Related posts:
 Indications of Tunnel Technique
Indications of Tunnel Technique
 Principle of Digestive Endoscopic Tunnel Technique
Principle of Digestive Endoscopic Tunnel Technique
 Tunnel Technique for SMTs Originating from Muscularis Propria
Tunnel Technique for SMTs Originating from Muscularis Propria
 Tunnel Technique for Digestive Mucosal Lesions
Tunnel Technique for Digestive Mucosal Lesions
 Techniques in Tunnel Establishment
Techniques in Tunnel Establishment
 Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Prevention and Treatment for Complications of Endoscopic Tunnel Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


