Kidney stones >2 cm
Cystine kidney stones ≥1.5 cm
Lower pole stones >1.5 cm or with an unfavourable infundibular angle
Stones in anatomical abnormalities suitable for percutaneous resolution (calyceal diverticula, ureteral stenosis, recurrence after UPJ stenosis surgery)
ESWL-refractory stones when RIRS is not suitable for difficult retrograde approach
In the end, the indications are substantially identical to adults, in the absence of congenital urinary malformations requiring open or laparoscopic reconstructive surgery, but the child safeguard needs the following essential requirements:
1.
Minimal invasiveness (small calibre of the endoscopes).
2.
Minimal anaesthetic time.
3.
Minimal X-ray exposure.
4.
Maximal stone clearance in one session.
5.
Shortest duration of post-operative drainage (possibly tubeless PNL), leading to more comfort and less pain.
17.4 Operative Armamentarium
17.4.1 Endoscopes
The instruments are the same as in adult procedures but with reduced calibre and length. It’s mandatory to have all paediatric endoscopic sets for performing PNL in a child, especially if aged <3 years.
There are semirigid ureteroscopes with a very small calibre on the market (like the Wolf 4.8 Ch), allowing to enter virtually any ureter, even the smaller ones. The harmless shape of the tip of the ureteroscope, exactly as in the adult, is an essential feature of such instruments (see Chap. 12). The new generation of semirigid ureteroscopes includes 7 Ch instruments with a large 4.8 Ch operating channel, sometimes suitable also for older children and adolescents as well as for adults (Fig. 17.1).
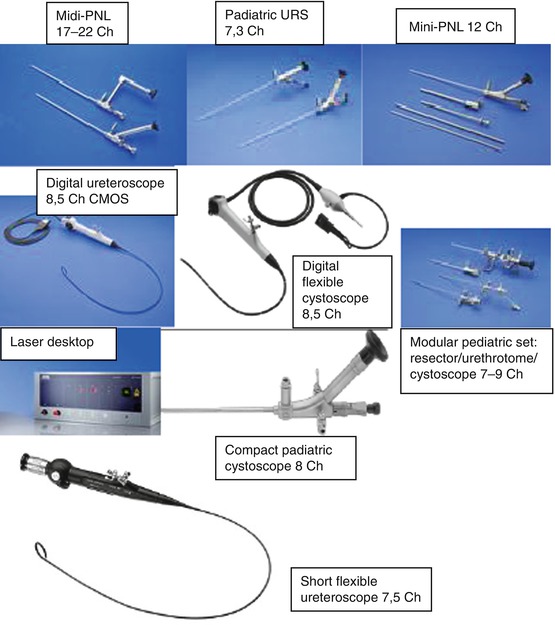
Fig. 17.1
Endoscopes used in a paediatric setting (RIRS/PNL)
Also flexible ureteroscopes, representing an important support for all percutaneous/endoscopic maneuver, need to be suitable for paediatric urinary systems in terms of calibre and length. In our department, we use standard 7.5 Ch Flex-X2 ureteroscope by Storz, allowing also the paediatric approach, upon application of a very small ureteral access sheath (9.5 Ch) when possible (Fig. 17.1).
As to the nephroscopes, those used for mini-PNL can be very handy, since their calibre is 12 Ch and their operative channel allows the introduction of ballistic probes and laser fibres, the intracorporeal lithotripsy energies most commonly employed during this kind of procedure. Larger nephroscopes (17–20 Ch) may also be used, when a 24 Ch Amplatz sheath can be applied.
As to the flexible instruments, both nephroscopes and ureteroscopes also in their digital version can be used, depending upon the diameter of the Amplatz sheath.
Warmed irrigation fluid should be used for all the endoscopes. In fact, another relevant issue in the child is hypothermia. Being their body so small, heath dispersion takes place much quicker than in an adult; thus, the anaesthesiologist will take care of covering the child with warmers and the urologist to use heated irrigation fluids (except during ultrasound lithotripsy, to avoid overheating), measures which are mandatory especially if PNL duration is 60–90 min.
17.4.2 Dilation Set
The usual percutaneous renal access in very small children is commonly the one called mini-PNL. In the mini-percutaneous approach, a Teflon coaxial dilation is used in order to achieve the 14/19 Ch Amplatz calibre (e.g. MIPP set – Rüsch – is a dedicated set with three coaxial hydrophilic dilators and a 14 Ch inner/19 Ch external Amplatz sheath). The mini-PNL set conceived by U. Nagele for Storz may also be employed, as well as a pneumatic set for dilation of the renal access (18–24 Ch Cook pneumatic balloon set or larger ones by Cook or Boston).
The leading concept of operative endoscopy, i.e. that instruments and access must adapt to the collecting system anatomy of the patient and not vice versa, is valid for the child even more than in the adult. In fact, any damage (including bleeding or urinary extravasation) may cause long-term consequences which may become difficult to manage with time.
The choice of the Amplatz sheath should be modulated on the calibre of the instruments we want to use in order to leave some space between Amplatz and endoscope, allowing the irrigation fluid to pour out freely, avoiding dangerous high intrarenal pressures, septic risk and liquid resorption. In fact, even minimal fluid resorption may cause hydro-electrolytic alterations and relevant metabolic consequences in children. This is also the reason why we consider 60–90 min as the maximal duration of a percutaneous procedure in a child, in spite of all due precautions, and we rather prefer an early second look to a prolonged PNL.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


