Fig. 3.1
Laparoscopes of different sizes and viewing angles facilitate visualization. (a) A 10-mm 30° angled tip laparoscope. (b) A 5-mm flexible-tip laparoscope
A xenon (300 W) light source is connected via the rod-lens to project adequate lighting onto the operative field (Fig. 3.2). Alternatively, some laparoscopes have integrated light sources. The light is carried to the rod-lens via fiber-optic cables. When passing the fiber-optic light source cable on and off the operative field, care must be taken to avoid damaging the relatively fragile fiber-optic cables, as damage to these will result in diminished light output and therefore an inferior image. It is recommended that the camera control equipment be connected to digital recording and storage devices to permit documentation, to promote teaching, and for use of the video in research endeavors.

Fig. 3.2
Standard light sources are shown
Insufflator
An electronically controlled carbon dioxide insufflator is used to establish and maintain pneumoperitoneum (Fig. 3.3). This system consists of the following: an intra-abdominal pressure display, an adjustable pressure selector, and digital flow and volume displays. Once pneumoperitoneum is initially established, high flow settings (20–40 L/min) are generally used to maintain the pneumoperitoneum. The system self-regulates to maintain the desired pneumoperitoneum.

Fig. 3.3
A standard insufflator permitting pneumoperitoneum for laparoscopic and robotic operations is shown
Instruments
A number of instruments have been designed specifically for use during laparoscopy. Many come in both reusable and disposable forms. The basic instruments that we advise having available for minimally invasive operations are the following:
Suction–irrigation device – this device allows for rapid intraoperative aspiration of blood, fluid, spilled bowel contents, etc., and/or irrigation of the same should the need arise.
Laparoscopic warmers – this allows one to keep the rod-lens device warmed to 37–40 centigrade in a saline bath to prevent fogging upon insertion into the warm, humid confines of the peritoneum. Having an antifog solution (Dr. Fog, Aspen Surgical MI, USA; Fred, Cardinal Health, OH, USA) available on the operative field can also facilitate rapid lens de-fogging. Newer laparoscopes, which have antifog features built into the rod-lens system, are available which eliminate the need for these baths.
Trocars – a variety of 5-, 10-, and 12- mm trocars are available. While the number and type depend on surgeon’s preference as well as the particular case being performed, we generally recommend having several 5- and 12-mm trocars readily available. Blunt tip trocars should be used to decrease the risk of injury to either the intestines or the abdominal wall musculature. The older, bladed trocars should be avoided [11].
Graspers (bowel and heavy graspers) – graspers are available in various sizes (5 mm and 10 mm), lengths (31 cm is standard), and shapes. Generally atraumatic (bowel), toothed, Maryland, Babcock, and right-angle graspers are the most useful for performing laparoscopic colorectal surgery.
Scissors – scissors permit both blunt and sharp dissection. Additionally, most can be connected to monopolar cautery, permitting improved hemostasis during dissection.
Clip applier and Endoloop – having a laparoscopic clip applier and Endoloop readily available in order to gain control of blood vessels prior to transection or in the emergent setting when rapid control of bleeding is desired is recommended.
Staplers – a variety of disposable laparoscopic staplers have been designed and are available in order to facilitate bowel and vessel transection as well as bowel anastomoses. Depending on the case, linear anastomotic staplers or circular end-to-end anastomosis staplers may be needed.
Energy sources – monopolar and bipolar sources of energy, as well as thermal dissecting devices, are available and are an important complement to the armamentarium of a laparoscopic colorectal surgery. Electrosurgery as well as LigaSure (Covidien, CO, USA), Enseal (Ethicon Endosurgery, OH, USA), and Harmonic scalpel (Ethicon Endosurgery, OH, USA) style devices greatly facilitate bowel surgery, specifically division of blood vessels within the mesentery and omentum.
Hand-Assist Techniques
Another technique for minimal access surgery is via a hand-assist technique. As with straight laparoscopy, laparoscopic instruments are used as well as a laparoscopic camera. A hand-assist port (GelPort Laparoscopic System, Applied Medical, USA) is inserted through a 6–7 cm abdominal wall incision through which the surgeon can pass one hand. The surgeon’s hand is then used to retract, dissect, etc. as needed.
Single-Port Techniques
A single-incision technique is also available wherein a 2–3 cm incision is made through the abdominal wall and a single-port device is inserted (GelPoint, Applied Medical, USA; TriPort and QuadPort, Olympus, Japan; SILS Port, Covidien, USA; Single Site Laparoscopic Access System, Ethicon Endosurgery, USA). All ports/instruments as well as the camera are inserted through this port and the procedure is completed without further incisions.
Robotic Techniques
Most robotic operations are hybrid techniques that involve the concurrent use of laparoscopic and robotic instruments. As such, availability of the laparoscopic instruments described in the prior section is essential to robotic cases. In addition to this, however, there are several robot-specific technologies which merit review.
The da Vinci robotic surgical system (Intuitive Surgical, Sunnyvale, USA) is the only robotic system currently available for surgical use. The system consists of a three- or four-armed surgical robot that docks into position at a desired location adjacent to the patient. The initial setup requires obtaining intraperitoneal access as would be done for laparoscopic surgery. Thereafter, a 12-mm endoscopic port is inserted, which permits initial laparoscope and later robotic laparoscope placement. Three reusable robotic instrument ports (8 mm) are then placed intraperitoneally. Each of the ports is configured so that it can be docked to the robotic arms. The robotic camera contains two separate video chips to allow for a binocular image. It is introduced through the 12-mm trocar and captures three-dimensional video of the intraperitoneal contents. These images are then projected to a control console placed some distance away from the patient. The surgeon sits at the console and is able to remotely control the camera and the robotic instruments connected to the arms of the da Vinci robot. An assistant (who is scrubbed in) is required at the patient’s bedside to exchange robotic instruments when necessary and to assist with retraction and suction if needed. The robotic instrument attachments most commonly used are a grasper, shears attached to monopolar cautery, and a bipolar grasper. The main advantages of robotic surgery over laparoscopic surgery are felt to be (1) the superior three-dimensional images that can be obtained of the intraperitoneal contents using the robotic endoscope and (2) the freedom of movement and motion that the robotic instruments allow for. The later is particularly useful when performing complex tasks (i.e., dissecting or suturing) within anatomically confined space. An ongoing randomized trial comparing laparoscopic and robotic surgery for rectal cancer will shed more light on the comparison of the two techniques [12].
General OR Setup for Minimal Invasive Colorectal Surgery
Figure 3.4 demonstrates a typical operating room setup for laparoscopic colorectal surgery. When available, ceiling-mounted booms help keep the various cords organized. We recommend that all cords and tubing enter and exit the sterile field from the same position whenever feasible. For example, for a laparoscopic low anterior resection, all tubes and cords could exit from the left side of the patient above the operative field. Figure 3.5 demonstrates a typical operating room setup for robotic colorectal surgery.
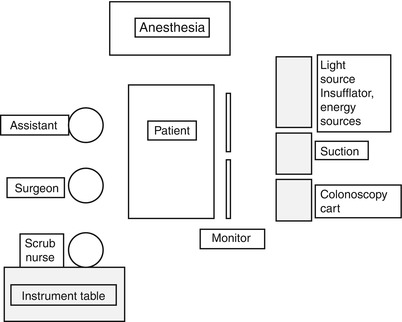
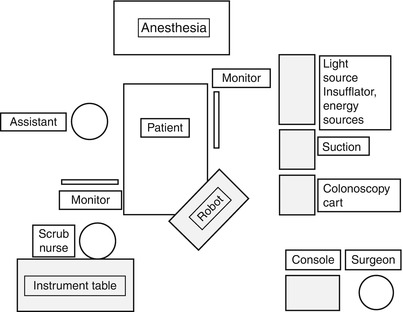
Fig. 3.4
Operating room setup for laparoscopic colorectal surgery
Fig. 3.5
Operating room setup for robotic colorectal surgery
Patient Positioning
In the following section we will discuss general patient positioning for the most common laparoscopic and robotic operations. We will defer discussion of port placement to subsequent chapters of this textbook, which will elaborate upon this topic in detail.
Regardless of the type of operation that is to be performed, a few principles should be kept in mind. First, the patient must be positioned is a manner that precludes pressure or nerve-related injury. All pressure points must be adequately padded and cushioned. Second, the patients should be secured to the operating table and prevented from sliding off the table. This is particularly important in laparoscopic and robotic surgery, where the surgeon may need to incline, turn and recline the patient at extreme angles to facilitate the operation. At our institution we use the Pink Pad – Pigazzi Patient Positioning System (Xodus Medical, PA, USA) – which consists of a single use pink foam pad placed directly on top of the operating table, disposable liftsheet, and body strap – to achieve this objective (Fig. 3.6). Alternatively, the patient can be positioned on a beanbag secured to the operating room table or a gel pad without liftsheets and shoulder pads. Third, all patients must have appropriate IV lines, cardiac monitoring leads, and catheters (including a urinary catheter permitting monitoring of intraoperative urine output) positioned in such a manner that they do not obstruct the surgeon’s operative field. Finally, appropriate prophylaxis (IV antibiotics, sequential compression devices, and/or chemical deep venous prophylaxis) must be instituted prior to initiation of the operation and continued/repeated as needed during the operation.

 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Robotic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
 Transanal Endoscopic Surgery (TES)
Transanal Endoscopic Surgery (TES)
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach
 Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach




Related posts:
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
Transanal Endoscopic Surgery (TES)
Proctectomy: Total Robotic Approach
Sigmoid Colectomy and Left Hemicolectomy: Single-Port Laparoscopic Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
