Fig. 4.1
Robotic surgeons console and hand console. For Fig. 4.1: provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)

Fig. 4.2
Robotic surgeons console and hand console. For Fig. 4.2: provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)

Fig. 4.3
Robotic surgeons console and hand console. For Fig. 4.3: provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)

Fig. 4.4
Dual robotic surgeon’s console. Provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)
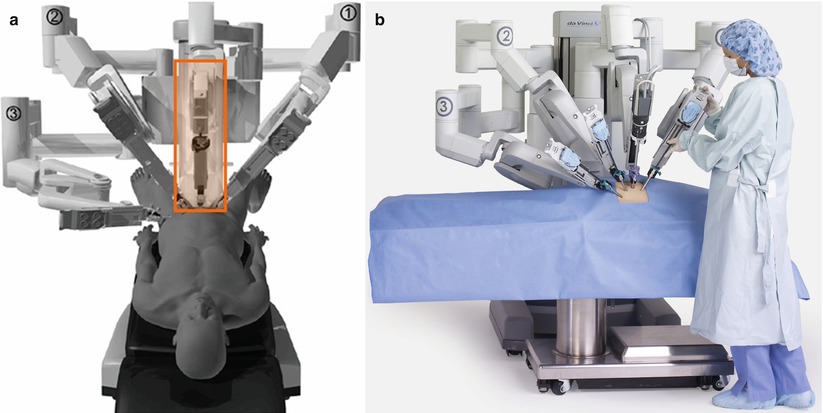
The patient side cart equipped with remote manipulator arms is controlled from the console by a surgeon. The remote manipulator arm is designed to move at the same time just like the surgeon is manipulating hand switches. Surgeons can perform a wide range of procedure, such as cutting, suturing, and electrocoagulation through the manipulator (Figs. 4.5 and 4.6).


Fig. 4.5
Patient side cart. For Fig. 4.5: provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)
Fig. 4.6
Patient side cart. For Fig. 4.6: provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)
The visualization system provides a panoramic view of the surgical field with high-resolution 3D images. The input to the surgeon’s monitor is generated by a stereo-endoscopic vision system that includes the camera, electronics, and a separate monitor for the operating team and assistants (Figs. 4.7a, b and 4.8).


Fig. 4.7
Robotic camera and camera arm. (a) Robotic camera, (b) robotic arm
Fig. 4.8
Wristed motion of robotic instruments. Provided here exclusively for promotion and/or media coverage of Intuitive Surgical and its products. This notification serves as an authorization for publications to make duplicate copies of the available high-resolution scans for editorial use only (© 2014 Intuitive Surgical, Inc. All people depicted unless otherwise noted are models)
Instruments are operated through small incisions in the body through which a robotic trocar is placed. There are various types of instruments designed to provide surgeons with natural dexterity and full range of motion for precise operation. The full range of motion and rapid responsiveness facilitate procedures such as suturing, knotting, dissection, and tissue manipulation. Many of the instruments used for robotic surgery mimic those that are available for laparoscopy (Figs. 4.8 and 4.9).
Fig. 4.9
Laparoscopic instruments (left) and robotic instruments (right) used for bowel surgery
General OR Setup for Robotic Surgery
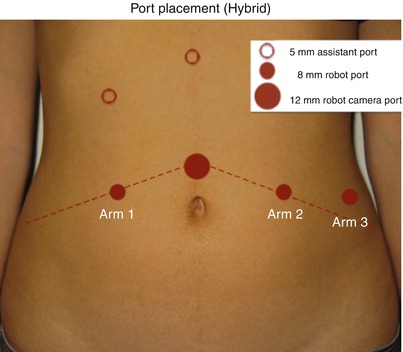
Setup of the robot is perhaps one of the most challenging aspects of robotic surgery. Early data has cited length of time to setup as a drawback of robotic surgery; however, once the team is efficient at this part of the procedure, the literature suggests that the operating times for laparoscopic and robotic colorectal procedures are similar [2]. Setup proceeds through various processes, according to the procedure and surgeon preference. First, after turning on the robot, calibration is essential for successful operation without delay or conversion. Often this setup is done prior to the surgeon or patient entering the room. It is necessary to calibrate the camera, patient side manipulators, and the master manipulators. If preparation for operation is finished, trocar locations need to be placed properly without “fighting” each other during operation, which results in collisions. The trocars should not be placed too close to each other. It is recommended by the manufacturer that each trocar site should be 8–10 cm apart to avoid collision and maximize arm excursion (Fig. 4.10) (Box 4.1) [3]. In addition, approximately 10–20 cm is the ideal distance between the trocar and target anatomy. Robotic trocars need to be inserted up until the thick black line can be visualized at the level internal surface of the cavity, which is the axis of rotation called the remote sensor (Fig. 4.11a, b).
 Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
 Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
 Right Hemicolectomy and Ileocecectomy: Robotic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
 Transanal Endoscopic Surgery (TES)
Transanal Endoscopic Surgery (TES)
 Proctectomy and Rectopexy: Laparoscopic Approach
Proctectomy and Rectopexy: Laparoscopic Approach
 Proctectomy: Total Robotic Approach
Proctectomy: Total Robotic Approach




Fig. 4.10
Robotic port placement hybrid technique for rectal dissection
Related posts:
Right Hemicolectomy and Ileocecectomy: Robotic Intracorporeal Anastomosis
Right Hemicolectomy and Ileocecectomy: Single-Port Laparoscopic Approach
Right Hemicolectomy and Ileocecectomy: Robotic Approach
Transanal Endoscopic Surgery (TES)
Proctectomy and Rectopexy: Laparoscopic Approach
Proctectomy: Total Robotic Approach
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
