Manometry (Esophageal)
(Gastroenterology. 2005;128:207-08 & 209-24. Gut 2001;49:145-51)
INDICATIONS:
Dysphagia not explained by stenosis or inflammation, Chest pain not explained by heart disease, Before fundoplication to exclude achalasia See also Esophagus/Gastric- Schatzki’s Ring (Chapter 1.22)
GENERAL/NORMAL: (Fig. 1.17.1A)
The Basal LES (tonically closed) at rest with a normal mean pressure of 20 mmHg (range 10-45 mmHg)
A wet swallow can alter subsequent swallows for up to 20-30 seconds, so it is important to note time intervals between swallows
After a wet swallow, Peristaltic wave progression occurs at a rate of 2-8 cm per second
Following peristalsis there is complete LES relaxation to allow bolus to pass (pressure drops to <8 mmHg above gastric pressure)
The normal Distal wave amplitude is 30-180 mmHg
Asymptomatic esophageal manometric findings should be ignored; Symptoms may not respond to therapies that correct abnormalities
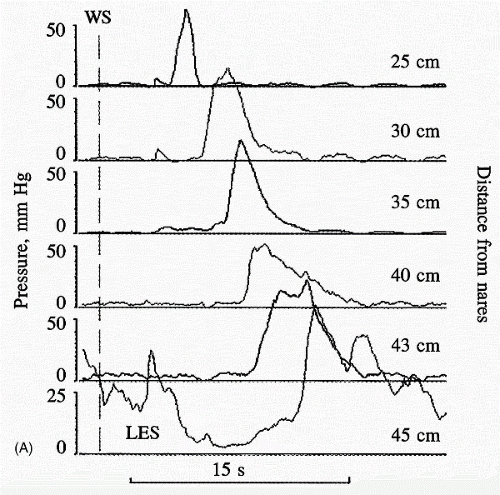 Figure 1.17.1 A. Normal esophageal motility. Reprinted from Talley NJ. Normal and abnormal esophageal motility. In: Hauser SC Ed. Mayo Clinic Gastroenterology and Hepatology Board Review 2nd ed. Mayo Clinic Scientific Press. 2006:37,38,40 with permission. |
ACHALASIA (Fig. 1.17.1B)
Basal LES: Usually high/>45 mmHg (may be normal) | LES relaxation: Incomplete (residual >8 mmHg) |
Peristaltic wave progression: Absent or simultaneous with identical configurations | Distal wave amplitude: Low or low-normal (<40 mmHg) |
Intraesophageal pressure can be increased because the esophagus is accommodating and behaving as a common cavityRelated posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



