Institution/country
Authors year
Relative contraindication
Absolute contraindication
Leeds United Kingdom
Mirnezami et al. 2010 [26]
Distant metastasis
Encasement of external iliac vessels
Primary stage IV disease
Extension of tumor through sciatic notch
Extensive pelvic sidewall involvement
Presence of lower limb oedema from venous or lymphatic obstruction
Predicted R1 or R2 resection
Poor performance status
Sacral invasion above S2-S3 junction
Boyle et al. 2005a [5]
Presence of extensive abdominal or thoracic metastases
Encasement of external iliac vessels
Extension of tumor through sciatic notch
Sacral invasion above the level of S2–3 junction
Lund Sweden
Zoucas et al. 2010a [35]
Adherence or invasion of sacrum at or above S2 level
Extensive lateral or circumferential pelvic wall involvement
Encasement of sciatic notch or external iliac vessels
Presence of unresectable distant metastasis
Texas United States
Ureteral obstruction
Distant metastases
Poor candidate for surgery because of medical comorbidities
Involvement of common or external iliac vessels
Poor candidate for surgery because of inability to care for stomas or senility
Metastasis to para-aortic nodes
Involvement of the sacrum proximal to S1 (note: some consider S2 involvement to an absolute contraindication)
Tumor extension through sciatic foramen
Pelvic sidewall involvement
Washington United States
Ogunbiyi et al. 1997 [22]a
The authors defined resectable disease as
Midline posterior tumors adherent or invading the distal sacrum below S2
Isolated perianastomotic or perineal recurrence
Tumors invading adjacent pelvic structures such as bladder, prostate or vagina
Absence of invasion of lateral pelvic sidewalls, upper sacrum and pelvic nerves (ad indicated by neurologic signs and symptoms)
No involvement of ureters as indicated by absence of hydronephrosis on imaging
Due to the associated surgical morbidity and mortality, pelvic exenteration is generally only offered with a curative intent. Patients with unresectable metastases are therefore not usually considered for pelvic exenteration. However, the presence of synchronous resectable visceral metastases or a history of previously treated metachronous metastases should not preclude consideration for pelvic exenteration provided the patient is medically fit for the procedure [32, 33]. Whether metasectomy and pelvic exenteration should be performed as staged or synchronous procedures and whether a metasectomy first approach is more appropriate is debatable, although synchronous procedures are likely to prolong surgical time and increase surgical morbidity considerably if a major resection is necessary.
Traditionally, pelvic sidewall recurrence was considered a formidable surgical challenge that is incurable [22, 34]. The potential involvement of major neurovascular structures essential for lower limb function coupled with the difficulties in achieving R0 resection margin have contributed to pelvic sidewall recurrence being considered a contraindication for surgical exploration [22, 35–37]. In fact, prior to the advent of MRI, referred pain in the distribution of the sciatic nerve alone was enough to preclude consideration for surgery [38, 39]. However, with improved understanding of pelvic anatomy and surgical technique, pelvic sidewall dissection has become standard practice in many centers [31]. A systematic approach to the pelvic sidewall as described by Austin and Solomon has been shown to achieve R0 resection margins in 53 % of patients with pelvic sidewall involvement, which is comparable to R0 resection rates at other sites of recurrence [6, 31]. Major iliac vessel excision and reconstruction, adopted from allied surgical specialties in the treatment of retroperitoneal soft tissue sarcomas has demonstrated that en bloc iliac vessel excision and reconstruction can improve R0 rates with acceptable morbidity and graft patency rates [40, 41]. En bloc excision of sciatic nerve, where necessary to achieve R0 resection margins is a well established practice in the sarcoma literature with better than anticipated functional outcomes [42–44]. Patients typically require a foot brace to prevent foot drop but mobility is acceptable. Although patients report mild to moderate physical impairment, most prefer some degree of disability over amputation [42].
To enable even more radical resections of the pelvic sidewall for tumors extending through the sciatic notch, Nielsen et al. recently reported on their initial experience with external hemi-pelvectomy (hind quarter amputation) on eight highly selected patients with a variety of locally advanced or recurrent pelvic malignancies [45]. External hemi-pelvectomy is highly morbid procedure that is generally reserved for malignant sarcomas of the pelvis but where possible, a limb preserving form of hemi-pelvectomy (internal hemipelvectomy) with bony reconstruction is favored [46]. Although hemi-pelvectomy has been reported sporadically for carcinomas of the pelvis, unlike sarcomas, its role in carcinomas remains unclear [45, 47–50]. Oncological outcomes following hemi-pelvectomy in general are poor and longer term follow up data is scant [45, 47]. In the absence of long term oncological and quality of life data, these procedures should only be offered in expert centers on an individual basis where lesser surgical interventions are not possible. Patients need to be counseled appropriately and ideally, surgical, oncological and longitudinal quality of life outcomes in these patients should be assessed to further define the role of hemi-pelvectomy in LARC or LRRC.
En bloc sacrectomy may be required in 9–24 % of all pelvic exenterations in order to achieve R0 resection margins [3–6]. Sacrectomies at or below S3 are generally classed as low sacrectomies whereas high sacrectomies involves sacral transection at the level of S1 or 2. High sacrectomies are associated with increased intra-operative blood loss, surgical morbidity and post-surgical neurological deficit [4, 51–53]. Although oncological and functional outcomes following sacrectomies for a range of skeletal and soft tissue tumors are well described, literature on sacrectomy for LARC or LRRC is much more limited [51]. While low sacrectomies are widely accepted because of comparable R0, survival and morbidity rates as those who do not require en bloc sacrectomy, [54–57] high sacrectomies were traditionally considered a contraindication for surgery [5, 22]. However, as with the paradigm shift with pelvic sidewall involvement, high sacrectomies are no longer a contraindication for surgery [53, 58, 59]. In a recent study by Milne et al. which included 21 patients who underwent en bloc S1/S2 sacrectomy for LRRC, R0, median and 5 year survivals of 74 %, 59 months and 38 % were reported respectively [53]. In another study by Dozois et al. on high sacrectomy for LRRC, an R0 rate of 100 % and a 5 year survival of 30 % were reported [58]. Importantly, post-operative function seemed good with the former study reporting no difference in neurological deficits between low and high sacrectomy patients and the latter reporting acceptable post-operative ambulation, function and improved pain control [53, 58]. Although more studies are needed, favorable oncologic outcomes coupled with an acceptable morbidity profile and functional outcome necessarily means that high sacrectomy should no longer constitute a contraindication for surgery.
Rarely, pelvic exenteration may be considered for palliative purposes. These are typically patients with symptoms that cannot be adequately palliated using alternative treatment options such as uncontrolled enterovaginal or vesical fistulae, offensive fungating tumors or patients with intractable pain [22, 60]. Several small and highly selected case series have reported dramatically improved symptom control [17, 60, 61]. Naturally, such radical approach to palliation carries the risk of bringing forth the patient’s demise but this also highlights the importance of quality of life and patient choice in decision making.
52.6 Treatment
Multi-disciplinary Team Approach
Treatment decision for LARC or LRRC patients should be made in a multi-disciplinary setting. These meetings should include all relevant surgical and medical specialties as well as allied health specialists such as cancer coordinator, stomal therapists and psych-oncologists. These meetings are also useful for work force planning to ensure the necessary specialties are available on the designated operation day.
Pre-operative Chemoradiation
Patients who are radiotherapy naïve should undergo pre-operative long course chemoradiation [62]. The role of re-irradiation in patients previously irradiated patients is currently unclear [19]. Re-irradiation options include external beam radiotherapy, intensity modulated radiotherapy (IMRT) or intra-operative radiotherapy (IORT). IMRT is a relatively new radiotherapy technique that delivers differential radiation doses precisely to better conform to the three-dimensional shape of the tumor. In doing so, parts of the tumor can receive higher doses while protecting surrounding critical structures [63]. IORT can deliver a much higher biological dose directly to the tumor bed without increasing tissue toxicity but requires purpose built operating theaters to do so [19]. This seems useful where resection margins may have been compromised but this simply underscores the importance of an R0 resection margin [19, 64, 65].
The role of re-staging after chemoradiation is currently unclear although the consensus from an international collaboration, the Beyond TME collaboration, recommends restaging with MRI and PET to assess treatment response prior to exenteration (manuscript in preparation).
Compartments of the Pelvis and Dissection Planes
Conceptually, the pelvis can be divided into five compartments (Fig. 52.1). They are the central, anterior, posterior and the two lateral compartments. Each compartment overlaps at their periphery and are each centered on a different structure. The central compartment is centered on the tip of the coccyx, while the anterior, posterior and lateral compartments are centered on the urethra, the third sacral vertebra and the ischial spines respectively. The contents of each compartment are listed in Table 52.2. Within each compartment are different extra-TME dissection planes and this is illustrated in Fig. 52.2. With these in mind, the surgeon can then conceptualize the three-dimensional anatomy of the cancer so as to formulate a surgical plan when the pelvic MRI is reviewed with an experienced MR radiologist.
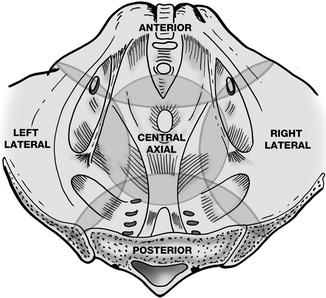
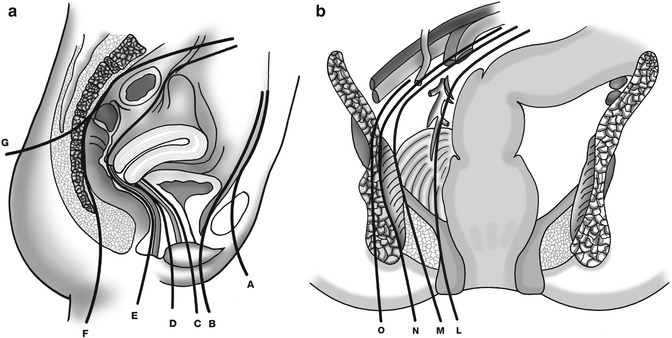
Fig. 52.1
Diagram of the pelvis illustrating the five pelvic compartments, each overlapping at their periphery. Each compartment is centered on a different structure with the anterior, central, posterior and lateral compartments centered on the urethra, the tip of the coccyx, the third sacral vertebra and the ischial spines respectively
Table 52.2
Contents within the compartments
Compartment | Viscera | Muscle | Bone | Others |
|---|---|---|---|---|
Anterior | Bladder | Obturator internus | Pubic symphysis | Dorsal venous complex |
Urethra | Obturator externus | Superior pubic ramus | ||
Males: prostate, seminal vesicles, vas deferens | Anterior pelvic floor (pubococcygeus, puborectalis part of levator) | Inferior pubic ramus | ||
Females: anterior vagina | ||||
Central | Females: posterior half of vagina, uterus, cervix, ovaries, fallopian tubes, broad ligament, round ligament | Pelvic floor muscles (iliococcygeus part o levator ani) | S4 and 5 sacral vertebra | |
Rectum | Coccyx | |||
Posterior | Rectum | Pelvic floor muscles (coccygeus) | Sacrum (S1-S5) | Branches and tributaries of the internal iliac vessels |
Piriformis | Coccyx | Sacral nerve roots (S1–S4) | ||
Anterior sacroccocygeal ligament | ||||
Medial sacrotuberous ligament | ||||
Sacrospinous ligament | ||||
Lateral | Ureter | Piriformis | Ischial spine | Internal iliac artery and vein |
Obturator internus | Ischial tuberosity | External iliac artery and vein | ||
Coccygeus | Obturator artery and vein | |||
Lateral sacrotuberous ligament | ||||
Sacrospinous ligament | ||||
Lumbosacral trunk | ||||
Sciatic nerve distal to ischial spine | ||||
Obturator nerve |
Fig. 52.2
(a) Sagittal section of a female pelvis demonstrating possible dissection planes. Plane A–G are the surgical dissection planes available. (b) Coronal section of a pelvis demonstrating possible dissection planes. Plane L is the TME plane; plane M is the extra-vascular plane which would involve excision of iliac vasculature; plane N is the plane that involves en bloc excision of obturator internus; plane O involves en bloc excision of ischial spine or ischial tuberosity
Surgical Technique
Pelvic exenteration is a heterogeneous group of operations where the specific procedure will vary depending on the location and the extent of the tumor. Because of this, there is no standardized surgical approach although broad principles can be applied. Of note, there is no universally accepted terminology for types of exenteration. Terms such as central, visceral, complete and total exenteration are often used interchangeably while others would use composite resection or abdominosacral resection to imply en bloc sacral resection. For clarity, exenteration is best defined as complete or partial based on the number of compartments excised.
All procedures can be subdivided into an exploratory phase, a dissection phase and a reconstructive phase. All procedures begin with an exploratory phase where the aim is to rule out occult metastatic disease that may preclude curative resection and to isolate the pelvic cancer from all small bowel loops by meticulous adhesiolysis, en bloc excision of contiguously involved small bowel loops and dividing the colon along its anatomical planes.
The aim of the dissection is to achieve a clear microscopic margin (R0). As a general principle, a compartmental approach is adopted whereby involvement of a compartment would necessitate complete excision of the compartment at its soft tissue bony junction or if the tumor extends very close to this margin, en bloc excision of the adjacent bone. Attempting to obtain a soft tissue margin in the former is likely to result in an unacceptably high rate of involved margins. In LRRC, the dissection planes are often poorly defined due to fibrosis from previous radiotherapy and total mesorectal excision. While detailed technical description of each exenteration procedure is beyond the scope of this chapter, it is important to highlight the modern breakthroughs in exenteration techniques.
Lateral Neurovascular Approach
Central to pelvic sidewall dissection is the appreciation that key neurovascular structures are organized in a “layered” manner where the ureter lies superficial to iliac arteries, iliac veins, lumbosacral trunk and obturator internus (Fig. 52.3). To gain access to a deeper structure, the superficial lying structure is dissected out so as to “float” it off the pelvic sidewall (Fig. 52.3). Lateral compartment dissection begins with ureterolysis and pelvic lymphadenectomy which facilitates vascular dissection and exposes the sacral plexus. The appropriate dissection plane is usually pre-determined by the staging MRI (Fig. 52.2). Where possible, the internal iliac artery should be ligated distal to the gluteal branches so as to reduce the likelihood of buttock claudication and to preserve the option of a gluteal artery based flap. Even where formal excision of the internal iliac vasculature is not necessary, in situ ligation of these vessels can help limit blood loss when a distal sacrectomy is planned.
Fig. 52.3
Intra-operative photo of pelvic sidewall demonstrating the right common, external and ligated internal iliac arteries (red vessel loops); the right common, external and ligated internal iliac veins (blue vessel loops); obturator nerve and lumbosacral trunk (yellow vessel loops). This photo demonstrates the “layered” organization of the lateral compartment neurovascular structures. Ligation of internal iliac artery and vein allows and common and external iliac systems to be “floated” off the pelvic sidewall
Dissection of the iliac veins is much more challenging due to the variable anatomy and thin walled veins. Loss of venous control is more commonly the cause of catastrophic bleeding in exenterative surgery. The surgeon can usually expect at least a visceral, spinal (or presacral) branch and a gluteal tributary at each level. Pre-emptive suture ligation after dissection of an appropriate venous cuff will ensure vascular control and progressively devascularize the pelvis. In LRRC, the extra-vascular plane is often virginal compared to the TME plane and may be comparatively easier to dissect even if vascular excision is not required.
Identification of the lumbosacral trunk is a key step in lateral compartment dissection as it leads to obturator internus muscle and ischial spine. Preserving the lumbosacral trunk for lower limb motor function is generally possible even if a distal sacrectomy is necessary. To completely excise the lateral compartment, obturator internus can be excised at its origin with or without en bloc excision of ischial spine or ischial tuberosity.
Anterior Compartment Dissection
Conventionally, the anterior dissection plane is the retro-pubic plane at the junction between bladder and pubic bone. As with the principles of en bloc bony excision in the lateral and posterior compartments to improve R0 resection, the same can be applied to the anterior compartment. In LRRC where there is extensive prostatic involvement or involvement of the membranous urethra following previous abdomino-perineal excision in men, en bloc pubic bone excision and excision of proximal penile urethra may be required to achieve a clear resection margin. In a study by Solomon et al. patients with LRRC who underwent en bloc cystectomy had a R0 rate of 64 % but this contrasts with an R0 rate of 100 % in patients who underwent en bloc cystectomy and pubic bone excision (pubic symphysis or bilateral inferior pubic ramus excision) when the membranous urethra was involved (manuscript in preparation). Although long term oncological data from pubic bone excision is not yet available, this demonstrates technique modification can further improve R0 resection rates. Of note, even if central pubic excision is performed, internal fixation is typically not required. Mesh reconstruction to the divided ends of pubic rami with overlying flap reconstruction is generally all that is required.
Posterior Compartment Dissection
The surgical approach for high versus low sacrectomy differ in that a high (S1/S2) sacrectomy generally requires a prone approach whereas a low sacrectomy (S3 and distal) can be performed via an abdominolithotomy approach. High sacrectomies can be highly morbid because division of proximal sacral nerve roots which can cause considerable lower limb motor and sensory deficits. Division of distal sacral nerve roots can result in an atonic bladder. Therefore, patients should be counseled appropriately about en bloc cystectomy even if it is not required oncologically. In patients where there is central involvement of L5 or S1, a central anterior table excision can be performed for L5 and S1 leaving the remainder of the sacrum intact thus preserving pelvic stability and sacral nerve roots.
Sacrectomy is usually the final step after completion of both the abdominal (lateral, anterior and other posterior dissections) and perineal phases of the procedure. This includes abdominal and perineal reconstruction where a prone sacrectomy is required. Posterior dissection begins in the TME plane but stops about 2 cm above the point where tumor adheres to sacrum. For distal sacrectomy, piriformis and sacral nerve roots are divided. After completion of the remainder of perineal dissection, the perineal surgeon disconnects gluteus maximus and tunnels immediately posterior to the coccyx and sacrum to the level of intended sacral division. A malleable retractor is then inserted to protect natal cleft tissue as the abdominal surgeon performs the sacrectomy using a 20 mm osteotome and mallet (Fig. 52.4).
Fig. 52.4
Distal sacrectomy performed via an abdominolithotomy approach using a 20 mm osteotome. Natal cleft tissues are protected with a malleable retractor
Where a prone sacrectomy is to be performed, to ensure that sacral transection is performed at the appropriate level, an orthopedic staple is secured into the sacrum 2 cm above the desired point of transection. The position of this staple is checked with intra-operative x-ray to confirm the point of sacral transection. It is also useful in these cases to have both lumbosacral trunks marked with a yellow vessel loop and a suture to orientate the rectus abdominis myocutaneous flap to avoid flap malrotation. Abdominal sponges are also left in the pelvis anterior to the sacrum to prevent small bowel from coming into contact with the anterior aspect of sacrum which may be inadvertently injured as the sacrum is being divided from the prone approach using an oscillating saw. Dural sac should be ligated in high sacrectomies to prevent ongoing cerebro-spinal fluid leakage.
Reconstruction
Consideration has to be given to visceral, abdominal and perineal reconstruction. Where cystectomy is performed, an ileal or colonic conduit will be required. Although ileal conduits are preferred, it may not be advisable in patients where small bowel loops have been heavily irradiated. A colonic conduit out of the radiation field may be associated with less complications in this setting [66]. The use of orthotopic neobladder reconstruction is popular within gynae-oncology literature [67, 68] but few are considering the technique in LARC or LRRC [69]. Where a segmental ureteric excision was performed, options include an end-to-end ureteric anastomosis, bladder re-implantation with a psoas hitch or nephrectomy. Re-implanting the ureter into the contralateral ureter or the use of a gastric or jejunal interposition graft are alternatives but the former is avoided if possible to prevent potential repercussions on both kidneys should surgical complications ensue.
In patients where a wide perineal excision or high sacrectomy has been performed, consideration needs to be given to reconstruction using a myocutaneous flap [70]. A rectus abdominis myocutaneous flap is the workhorse for this reconstruction as flap harvest can be incorporated to the laparotomy incision in addition to providing a bulky and well-vascularized tissue with a skin paddle for reconstruction. In patients with previous bilateral stomas, assessing patency of the inferior epigastric artery is recommended. Alternative tissue flaps include gluteal V-Y advancement flaps, inferior gluteal artery perforator based flaps or anterior thigh flaps [71–74]. It is important that skin paddle harvested is not excessive as this will only introduce donor site morbidity. If a rectus abdominis myocutaneous flap is harvested, mesh reconstruction of the abdominal wall will be necessary.
Related posts:
 Radical Cystectomy: Robotic, Laparoscopic, Open and Partial
Radical Cystectomy: Robotic, Laparoscopic, Open and Partial
 Diagnostic and Endoscopic Management of Bladder Tumors
Diagnostic and Endoscopic Management of Bladder Tumors
 Considerations for Management of Hereditary Rectal Cancer and Desmoid Tumors
Considerations for Management of Hereditary Rectal Cancer and Desmoid Tumors
 Training Surgeons for Rectal Cancer Surgery: Clinical and Simulation
Training Surgeons for Rectal Cancer Surgery: Clinical and Simulation
 Radical Hysterectomy in Cervical Cancer
Radical Hysterectomy in Cervical Cancer
 Imaging of Gynecological Cancers
Imaging of Gynecological Cancers
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


