| 21 | Management of Benign Strictures |
 Definition and Causes
Definition and Causes
Benign stenoses can be caused either by inflammatory healing processes involving scarring (mainly associated with Crohn disease, but also ischemic colitis and NSAID [nonsteroidal anti-inflammatory drug] colitis) or they may occur as postoperative stricturing.
Colitis. Stenosis is particularly common in fibrostenotic Crohn disease. Depending on the pattern of colon involvement, strictures can involve the terminal ileum, the Bauhin valve, or other colon segments. Strictures may appear with scarring and a smooth mucosa or they may also have variously deep ulcers if occurring in a phase of florid inflammation. Stricture formation has also been associated with rapid healing processes following intensive anti-inflammatory therapy (e.g., anti-TNF antibodies). Typically, stenosis formation has a predilection for the anastomosed region around ileocolostomies ( 21.1a, h). Stenosis in a confirmed diagnosis of ulcerative colitis, however, always raises the index of suspicion for malignancy and must be operated.
21.1a, h). Stenosis in a confirmed diagnosis of ulcerative colitis, however, always raises the index of suspicion for malignancy and must be operated.
The occurrence of strictures following ischemic colitis or NSAID colitis varies and the degree of severity is unpredictable. Chronic courses, in particular, can lead to symptomatic manifestation. Later stages of radiation colitis are often associated with strictures affecting longer segments.
 21.1 Balloon dilation of benign strictures
21.1 Balloon dilation of benign strictures

a–c Crohn disease. Inflammation and stenosis at ileoascendostomy (a). Advancement of a TTS balloon through the stenosis (b). Inflation of the balloon in the stenosis (c).
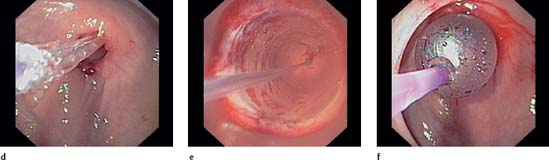
d–g Stenosis at anastomosis following sigmoid resection due to diverticulitis. Stenosis not passable. Advancement of the TTS balloon (d). Inflated balloon in the stenosis, filled with water and contrast agent. One can look through the balloon to the stenosis wall and to a certain degree see it dilating (e). Correct positioning of the balloon in the stenosis is controlled endoscopically during the entire procedure (f). In many cases, radiological surveillance is thus unnecessary.

g Final image after three sessions of balloon dilation. The stenosis is now sufficiently opened and endoscopic passage is possible. A few staples are visible at the edge.
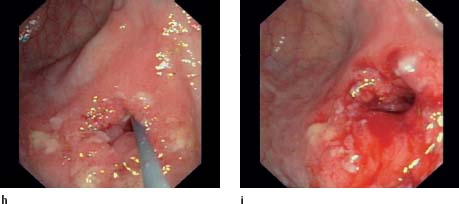
h, i Stenosis and inflammation of ileocolonic anastomosis in Crohn disease. “Laying out” the guidewire (h
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


