CHAPTER 3 MAJOR HEPATIC RESECTION: RIGHT LIVER
RIGHT HEPATECTOMY*
INFLOW AND BILIARY CONTROL
The hilar plate is opened to expose the left hepatic duct and the confluence of the bile ducts. The cystic duct and the cystic artery are exposed, ligated, and divided (Fig. 3-1), and the gallbladder is removed. The cystic duct is transfixed before being ligated, and a tie is left on the cystic duct for later retraction. Some surgeons now proceed to extrahepatic dissection of the right hepatic duct (see subsequent discussion); but this is not advisable. It is better to dissect the right hepatic artery and portal vein and to leave management of the right hepatic duct until later in the operation.
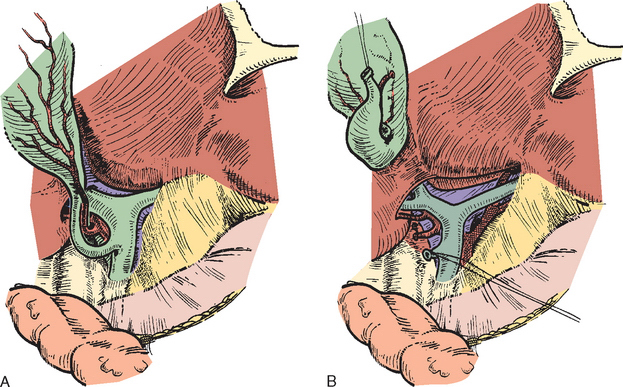
Figure 3-1 A, The peritoneum overlying the common bile duct and extending up into Calot’s triangle is incised. B, The cystic duct and cystic artery are secured. A tie is left on the cystic duct for later retraction (see text and Fig. 3-2). The hilar plate is lowered to expose the left hepatic duct and the confluence of the bile ducts.
The right hepatic artery is dissected, ligated, and divided. I deliberately double-suture ligate the proximal end and hold this after division for light traction to the left, which together with traction on the cystic duct stump is of assistance in exposing the portal vein (Fig 3-2).
The portal vein is approached laterally and posterior to the common hepatic duct. The main portal trunk is exposed, and the left branch is identified and preserved. Sometimes the right anterior and posterior sectoral branches of the portal vein arise individually (see Chapter 1), and these origins may be separated by as much as 2 cm (see Fig. 3-2).
Application of a straight-bladed vascular clamp is a safe method of transecting the right portal vein (see Fig. 3-2). If the vein is ligated, it should be transfixed and double ligated. The portal vein may also be divided using the Endo-GIA vascular stapler. If the right anterior and posterior sectoral branches arise independently (see Fig. 3-2), they require individual control. The hepatic bile duct or its major sectoral tributaries are usually secured in the pedicles (see the following) further laterally at the time of parenchymal dissection. However, deliberate dissection of the hepatic ducts must be carried out for tumors that approach the hilus of the liver.
The confluence of the bile ducts and the infrahepatic course of the left hepatic duct should be identified after lowering of the hilar plate (see Fig. 3-1). It may help to divide the liver tissue that occupies the lower limits of the umbilical fissure and bridges the gap between the quadrate lobe (segment IV) and segment III of the left liver. This maneuver opens the umbilical fissure and allows better exposure of the subhepatic and hilar area.
When the right hepatic duct is dissected, it should be transfixed, ligated, and divided (see Fig. 3-2). Difficulty might be encountered in passing an instrument around the right hepatic duct, in which case it may be divided under direct vision and subsequently oversewn with a 4-0 Vicryl suture (Vicryl; Ethicon, Edinburgh, UK) on an atraumatic needle. In many instances, the ducts draining the anterior and posterior right sectors are found entering the confluence separately, or the posterior sectoral duct may join the left hepatic duct (see Chapter 1). In such cases, both these major sectoral ducts should be individually identified and secured. It is again emphasized that extrahepatic dissection is not usually necessary for peripherally placed tumors. In such cases pedicular control is adequate.
CONTROL OF PORTAL PEDICLES
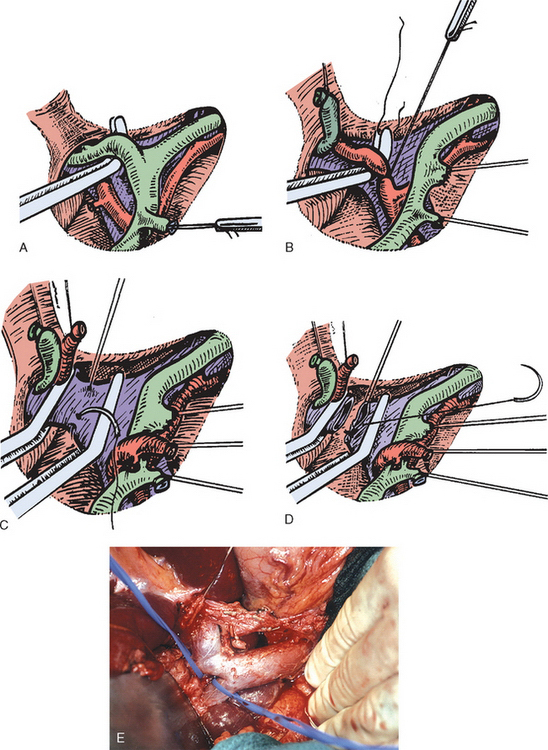
The structures of the portal triad carry Glisson’s capsules with them as they penetrate the liver and are contained in a well-formed sheath within the parenchyma (Fig. 3-3). The pedicular sheaths can be exposed after appropriate hepatotomies (Fig. 3-4) and are tough enough to be dissected, encircled, and clamped (Fig. 3-5).

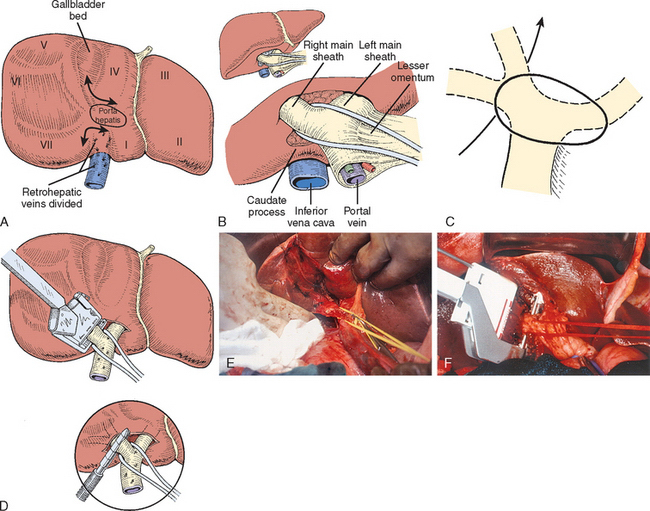
Figure 3-4 A, The approach to the right portal pedicle. The liver has been mobilized from the inferior vena cava by division of the retrohepatic veins lying behind the caudate process. Hepatotomies have been made in the region of the gallbladder fossa and the caudate process. The curved double-headed arrows indicate the sites of the hepatotomies above and below the porta hepatis. B, A vessel loop is drawn about the right pedicle and pulled to the left to protect the left pedicular structures during transection of the right main sheath. C, The arrow indicates the path of the finger (see Fig. 3-5) or instrument during dissection of the right pedicle allowing its isolation. D, The right portal pedicle is controlled and subsequently divided using a vascular stapler. E, Intraoperative photograph shows the right portal pedicle exposed by finger dissection and surrounded by a yellow vessel loop, which is drawn to the patient’s left (see also B). The vessel loop is drawn firmly to the left, and the pedicle is divided using the stapler as shown in D. F, Operative photograph shows division of the right portal vein pedicle, which is encircled by a red vessel loop pulled to the left. The vascular stapler is being used to divide the pedicle, as illustrated in D.
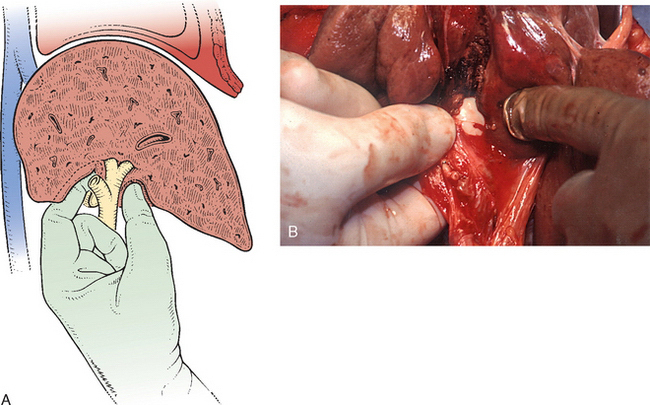
Figure 3-5 A, Illustration shows digital isolation of the right pedicle. B, Operative photograph illustrates insertion of the index finger through a hepatotomy in the caudate lobe where it merges with the base of the gallbladder fossa to isolate the right portal pedicle. A vessel loop is drawn about the pedicle as shown in Fig. 3-4.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


