Fig. 11.1
Omental pack. A graft of viable omentum is pulled through the penetrating tract in the liver
Penrose pack. Described by Bluett et al. [4], it involves using a pack of Penrose drains as a tamponading plug inside the long, penetrating tract. A long Kelly clamp is passed through the missile tract. A pack made of a collection of 0.5″ or 1″ Penrose drains is pulled back through the tract and left in the laceration (Figs. 11.2 and 11.3). The Penrose pack serves to exert gentle pressure on the surrounding hepatic parenchyma and controls the bleeding. The drains, brought to the exterior through the flank, also serve to drain the laceration. The drains may be “shortened” gradually over the next few days to allow the tract to collapse behind the receding drains. This technique facilitates hemostasis and helps to avoid a tractotomy or major resection in difficult circumstances.
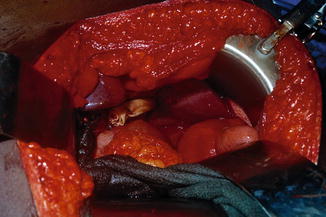
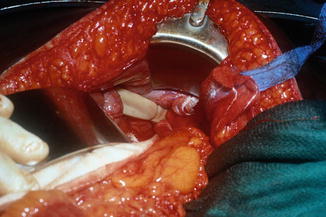
Fig. 11.2
Penrose pack through a bi-lobar transfixing gunshot wound of the liver
Fig. 11.3
The pack is pulled through the other surface of the liver and exteriorized as a drain
Balloon tamponade. As reported by Morimoto et al. [5], this therapeutic modality has shown to be effective and less traumatic than hepatotomy. Several methods are available for balloon tamponade. We have achieved intrahepatic balloon tamponade of missile tracts by using a sterilized Sengstaken-Blakemore tube (S-B tube). This tube, traditionally used for esophageal variceal bleeding, has a gastric balloon, a long esophageal balloon, and a lumen for drainage (Fig. 11.4). The sterilized tube is introduced into the long bi-lobar intrahepatic tract through a suitable point in the abdominal wall that is aligned to the tract, such that the esophageal balloon lies in the tract. It is then inflated with saline, enough to tamponade the tract and control bleeding. The balloon may be deflated over the next few days gradually as hemostasis is secured. Morimoto et al. [5] used a similar technique of balloon tamponade. The balloon can be “manufactured” in the operating room using a tube and a Penrose drain. The balloon consists of two drains arranged coaxially, an internal tubular one (no. 14 or 16 Levine tube or a red rubber catheter) and an external, laminar one of the Penrose type. The Penrose drain is firmly tied to the tubular one at the ends and the tube is occluded with a ligature at its distal end. The balloon portion should be longer than the intrahepatic tract by about 6 cm. The device is then introduced into the tract, leaving about 2–3 cm protruding from either end of the tract (Fig. 11.5). Video 13 illustrates the technique. The balloon is then inflated with saline enough to lie snugly in the tract and procuring hemostasis by gentle compression on the liver parenchyma. Some authors instill some radiopaque contrast material into the saline in the balloon, so it can be studied radiologically. The end of the tube is brought out to the exterior and serves as a drain. This usually controls bleeding and the balloon can be deflated gradually over the next week or so and eventually removed. Several successful series using the technique were published by Smaniotto et al. [6], Branco et al. [7], and others [8]. Poggetti et al. [9] succinctly described the procedure of intraoperative manufacturing of the balloon device and quoted their experience with more than 35 patients without failures or “breakthrough” bleeding. The advantages of using a tamponading balloon are the easy preparation of the device and the efficiency in obtaining hemostasis, with no need for major or more aggressive surgical procedures. In fact, Poggetti et al. [9] commented that they believed that many of the major injuries involved hepatic veins, and this technique may also control hepatic venous bleeding. While intrahepatic abscesses have been noted as a complication in a small number of cases, a direct cause and result to balloon compression has not been established.

 Acquisition of Surgical Skills by Hepatobiliary Rotation
Acquisition of Surgical Skills by Hepatobiliary Rotation
 Liver Trauma: Parenchymal Repair and Resectional Debridement
Liver Trauma: Parenchymal Repair and Resectional Debridement
 Parenchyma: Formal Lobectomy
Parenchyma: Formal Lobectomy
 Damage Control Laparotomy
Damage Control Laparotomy
 Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
 Acquisition of Surgical Skills in Animal and Simulation Laboratories
Acquisition of Surgical Skills in Animal and Simulation Laboratories




Related posts:
Acquisition of Surgical Skills by Hepatobiliary Rotation
Liver Trauma: Parenchymal Repair and Resectional Debridement
Parenchyma: Formal Lobectomy
Damage Control Laparotomy
Juxtahepatic Venous Injuries: Emergency Measures, Definitive Control, and Atriocaval Shunts
Acquisition of Surgical Skills in Animal and Simulation Laboratories
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
