CHAPTER 5 LIVER RESECTION: HEPATIC SEGMENTECTOMY
INTRODUCTION*
Segmental resection conserves functional liver parenchyma and minimizes the physiologic impact of liver resection. This is of particular benefit in a cirrhotic patient with impaired hepatocellular function. Segmentectomy may be regarded as a unisegmentectomy when one segment is removed or as a plurisegmentectomy when two or more segments are excised. More commonly performed segmental resections include resection of segment I; resection of segment IV; and segmentectomy to remove segments IV, V, and VI (Figs. 5-1 and 5-2). Central hepatic resection comprising resection of segments IV, V, and VIII is being increasingly performed, and this may be combined with resection of segment I, the latter operation being particularly indicated in some patients with hilar cholangiocarcinoma. Resection of segments VI and VII is, in effect, a posterior right sectorectomy, and resection of segments V and VIII is an anterior right sectorectomy.
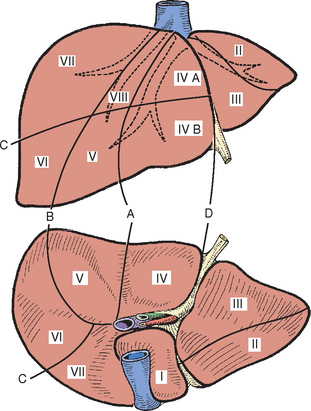
Resection of segment IV is of value in the management of malignant lesions occupying only the quadrate lobe. Carcinoma of the gallbladder is a special case because the organ lies between segments IV and V of the liver. Resection for gallbladder cancer should involve, as a minimum, removal of segments IVb and V. Resections of segments II or III (Fig. 5-3) are less frequently performed.
SEGMENTECTOMY I (CAUDATE RESECTION)
The procedure may be required as an isolated caudate lobe resection (Lerut et al., 1990) or as caudate resection combined with major hepatectomy (Bartlett et al., 1996). The anatomy of the caudate lobe and its close proximity to major vascular structures make resection difficult.
ANATOMY
The caudate lobe (segment I) is the dorsal portion of the liver posteriorly and embraces the retrohepatic inferior vena cava (IVC). The lobe lies between major vascular structures: the IVC posteriorly and the portal triad inferiorly and the IVC and the middle and left hepatic veins superiorly (Figs. 5-4 and 5-5). The anatomy is fully described in Chapter 1.
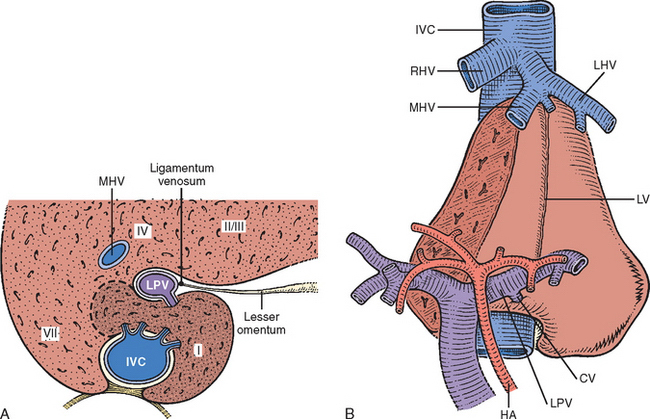
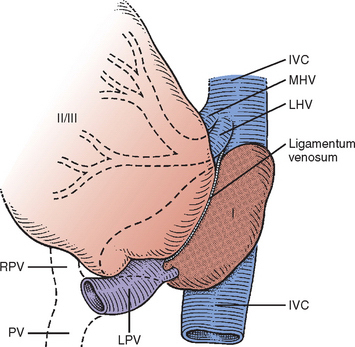
Figure 5-5 Sketch shows the position of the caudate lobe relative to surrounding structures, particularly the vena cava. Segments II and III have been rotated to the right to expose the caudate lobe. The position of the ligamentum venosum is indicated. Note the extension of the caudate lobe between the vena cava and the portal vein (PV) anteriorly and between the vena cava and the middle and left hepatic veins superiorly. Caudate portal blood supply is via a branch of the left portal vein (LPV). LHV, Left hepatic vein; MHV, middle hepatic vein; RPV, right portal vein (see also Fig. 5-4).
RESECTION
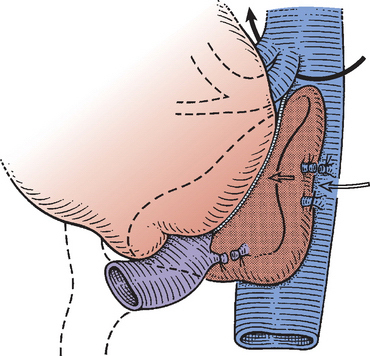
Dissection at the base of the umbilical fissure allows identification of the caudate vessels issuing from the left side of the portal vein and the left hepatic artery (Figs. 3-14, 5-6, and 5-7). The left lobe of the liver is mobilized and turned to the right. The left lateral margin of the caudate is freed by division of the fibrous extension of the tissue as it courses posteriorly to the IVC (see Fig. 5-4). This division allows access to the caudate veins (see Figs. 5-4 and 5-7). During this dissection, it becomes evident whether the caudate lobe is embracing the vena cava posteriorly and whether an approach should also be made from the right (see Fig. 5-7).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


