(1)
Department of Vascular Surgery, Evangelisches Krankenhaus Königin Elisabeth Herzberge, Berlin, Germany
10.1 Pathophysiology
The following experience is exclusively based on ePTFE prostheses. Their surface is uneven, fibrillary, and hydrophobic with pore sizes 50–70 μm, varying with the respective manufacturers. Only after exceeding a critical pressure may fluid permeate the wall. This pressure is called the hydrophobic barrier. According to manufacturers it is around 300 mmHg.
In practice, however, in some patients plasma leaks from grafts at much lower pressures. Our lab tests showed that the protein and electrolyte content of this leaking fluid corresponds to that of blood plasma. Consequently there is a filtration process rather than a tissue reaction to the prosthesis, but it may also be called perigraft reaction in so far as this filtration also leads to alterations of the surrounding tissue. This filtration is caused by the conversion of the ePTFE graft surface from a hydrophobic to a hydrophilic state brought about by plasma molecules.
Before 1992 when we started selective sequential fibrin sealing of the outer graft surface, we observed the intraoperative filtration of prostheses in almost a third of our dialysis patients. In patients who did not require hemodialysis, we could observe a clinically relevant filtration of non fibrin-sealed ePTFE grafts (peripheral bypass surgery) in around 1 %. Damage to the ePTFE wall and also to its potential fibrin coating (e.g., by clamping or grasping) favors filtration. As we take care to avoid this damage as much as possible, the experience reported here mostly refers to patients who had already been treated elsewhere.
The clinical presentation depends on the relation of the filtered volume (filtrate) to the absorptive capacity of the surrounding tissue and the duration of the filtration.
10.2 Clinical Presentation and Therapy
According to the clinical presentation and course we distinguish between five types of graft filtration.
10.2.1 Type I
Intraoperative filtration of small droplets (frequently only near the arterial anastomosis) (Fig. 10.1). After the wound closure, healing is usually not impaired as filtration tends to stop soon.
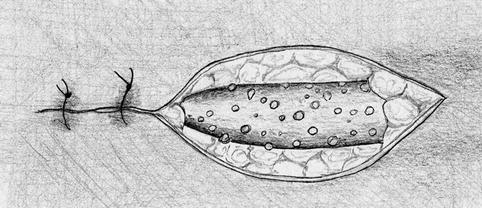
Fig. 10.1
Intraoperative findings. Loss of clear fluid through the graft surface
Frequency
Around 30 %.
10.2.2 Type II
Edema and slight erythema over the prosthesis lasting for days to weeks without (sonographic) proof of a fluid collection around the graft (Fig. 10.2).
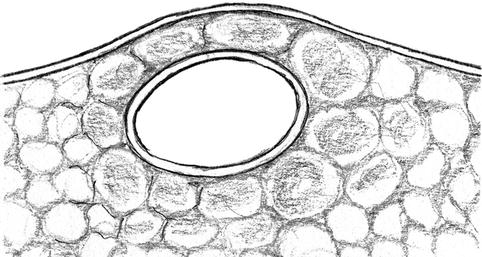
Fig. 10.2
Edema around the prosthesis
In this type, filtration persists for a longer time although the absorptive capacity seems to be sufficient. Differential diagnosis should include infections.
Frequency
10–15 %.
Therapy
Conservative with cooling and immobilization of the raised extremity.
No punctures as long as the edema persists.
Prognosis
After the edema subsides, complete healing can be expected. The time needed before we recommend the first puncture is significantly longer than usual.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


