Chapter 7 Laparoscopic Revision of Failed Fundoplication and Hiatal Hernia

Operative indications
Anatomic Failure
Seven types of anatomic failure may be encountered.
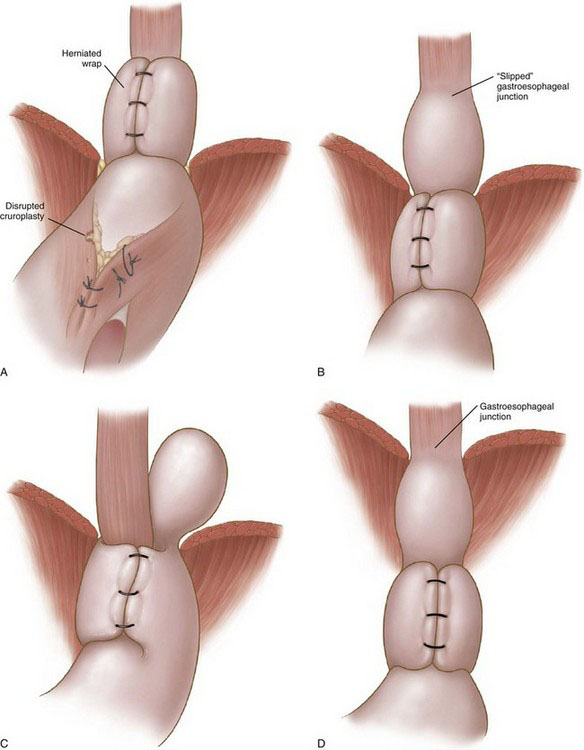
• Wrap migration (44%). A portion of the wrap or the entire wrap has migrated into the mediastinum (Fig. 7-1A). The proposed etiologic factor is inadequate crural closure owing to poor technique or weak tissue, or both; disruption of the cruroplasty results in migration of the wrap into the mediastinum.
• Slipped hernia (16%). The gastroesophageal junction has slipped into the mediastinum, whereas the wrap remains below the diaphragm (Fig. 7-1B). It has been postulated to result from the presence of a short esophagus or inadequate mobilization of the esophagus during the primary procedure. The latter is a more probable mechanism.
• Paraesophageal hernia (16%). Both the body of the wrap and the gastroesophageal junction remain below the diaphragm, whereas a part of the stomach has migrated into the mediastinum, posterior to the esophagus (Fig. 7-1C). This type of failure is a result of the combination of a loose wrap and a poor crural closure, which allows part of the posterior portion of the wrap to migrate into the mediastinum.
• Displaced wrap (10%). The wrap has slipped caudad on the body of the stomach, resulting in formation of a fundal pouch (Fig. 7-1D). The reasons for this type of failure are elusive; inadequate anchorage of the fundoplication may play a role. Retention of food in the herniated pouch may result in an increase of its size and further caudad slippage of the wrap (hourglass stomach).
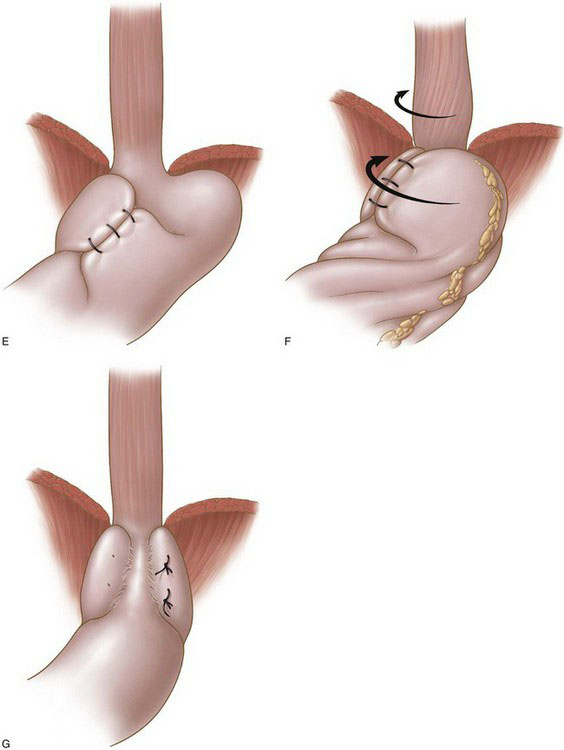
• Misplaced wrap (4%). The plication has been constructed by the fundus and the body of the stomach because of misidentification of the anatomy at the initial operation (Fig. 7-1E).
• Twisted wrap (6%). Torsion of the wrap is thought to result from insufficient division of the short gastric vessels and continuous traction counterclockwise (Fig. 7-1F).
• Disrupted wrap (4%). A part of the fundoplication or the entire fundoplication has been disrupted. Inadequate construction of the fundoplication (superficially placed sutures) may account for this failure (Fig. 7-1G).
Preoperative evaluation, testing, and preparation
Computed Tomography and Ultrasonography
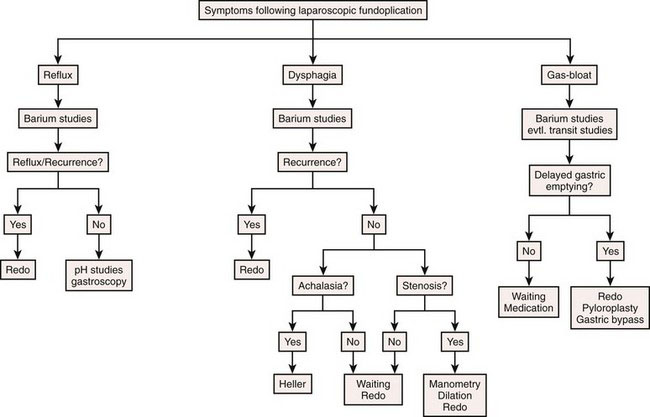
A diagnostic algorithm based on clinical history, patient complaints, symptom frequency, and severity is essential for the selection of suitable candidates for operative treatment and is presented in Figure 7-2.
< div class='tao-gold-member'>
Related posts:
 Laparoscopic Reversal of the Hartmann Procedure
Laparoscopic Reversal of the Hartmann Procedure
 Challenging Cases of Laparoscopic Enterectomy for Benign and Malignant Diseases of the Small Intestine
Challenging Cases of Laparoscopic Enterectomy for Benign and Malignant Diseases of the Small Intestine
 Laparoscopic Hysterectomy for Benign Conditions
Laparoscopic Hysterectomy for Benign Conditions
 Laparoscopic Colectomy for Diverticulitis
Laparoscopic Colectomy for Diverticulitis
 Laparoscopic Repair of Perforated Peptic Ulcer
Laparoscopic Repair of Perforated Peptic Ulcer
 Minimally Invasive Low Anterior Resection with Total Mesorectal Excision for Malignancy
Minimally Invasive Low Anterior Resection with Total Mesorectal Excision for Malignancy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


