Chapter 29 Laparoscopic Repair of Complex Scrotal Hernia

Trocar placement
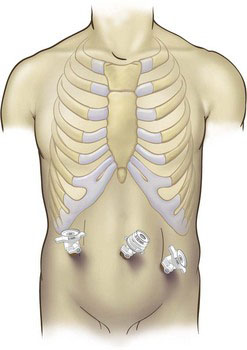
We prefer to access the abdomen using the open Hasson technique. A curvilinear incision is made inferior to the umbilicus, a 10-mm trocar is placed and the pneumoperitoneum is established. Two additional 10-mm trocars are then placed lateral to the rectus abdominis muscle at the same level as the infraumbilical port (Fig. 29-1).
Operative technique
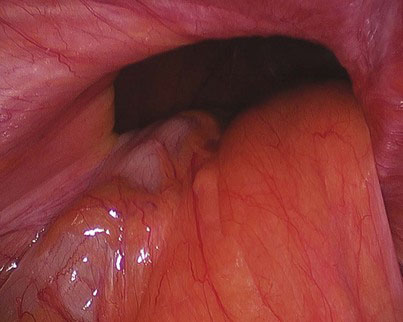
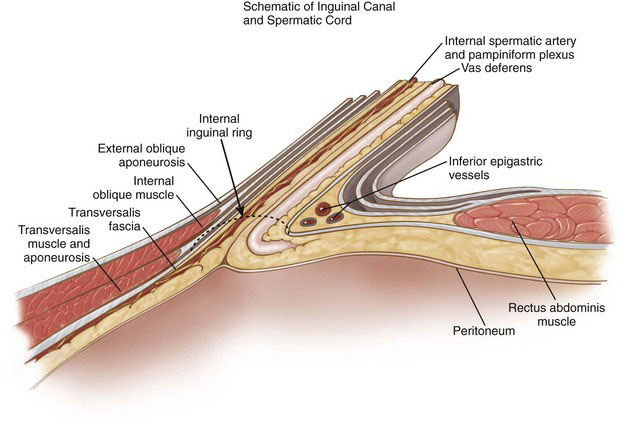
The patient is placed in Trendelenburg position to allow displacement of the small intestine and omentum from the lower abdomen, and the hernia defect is identified (Fig. 29-2). Using gentle traction, the hernia contents are reduced. External pressure on the scrotum may be used to facilitate the reduction. With large incarcerated scrotal hernias, the bowel can often become very adherent to the cord structures and sac. Care must be taken to avoid iatrogenic injury to the bowel wall and cord structures during reduction. Reduction of the sac should be attempted without performing intestinal adhesiolysis because the lysis of these adhesions only increases the chance for bowel injury. After the bowel is returned to the abdomen, the hernia sac is evaginated into the abdominal cavity with steady pressure elevating the peritoneum away from the anterior abdominal wall. This maneuver can be facilitated by inserting a grasper into the inguinal defect and grabbing the end of the hernia sac. With large hernias, the sac can be very adherent to the cord, making reduction difficult. If unable to fully reduce the sac, at this point it is better to open the peritoneum and complete the mobilization and reduction from the preperitoneal space. The peritoneum is opened above the inguinal ring using hook electrocautery from the median umbilical ligament to a point about 10 cm laterally. The inferior epigastric vessels are identified and preserved as they come up from the internal inguinal ring and course along the anterior abdominal wall (Fig. 29-3). The avascular plane between the peritoneum and underlying transversalis fascia is then bluntly dissected with a palpation probe or similar device, opening the preperitoneal space. Medially, the dissection is carried out until the Cooper ligament overlying the superior pubic ramus is clearly exposed. Often, a small blood vessel originating from the obturator artery is identified overlying Cooper ligament, and care must be taken to avoid injury to this vessel during dissection of the preperitoneal space or while anchoring the mesh in place.
< div class='tao-gold-member'>
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


