and Chao-Hui Zheng1
(1)
Department of Gastric Surgery, Fujian Medical University Union Hospital, Fuzhou, China
7.1 Review of Laparoscopic Cardial Area Lymph Node Dissection for Gastric Cancer
The lymph nodes (LNs) in the cardial area are located on both sides of the cardia and along the gastric lesser curvature. They include the No. 1, No. 2, and No. 3 LNs (Fig. 7.1). Complete dissection of the LNs in this area is also an important procedure during radical gastrectomy for gastric cancer.
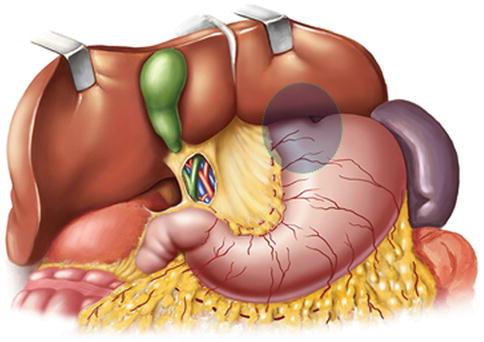
Fig. 7.1
Cardial area
There is a higher frequency of No. 1 or No. 3 lymph node metastasis (LNM). The common metastatic pathway is from No. 3, No. 1, No. 7, to No. 9, wherever the tumor is located in the upper, middle, or lower third stomach. No. 1 and No. 3 LNM are correlated to tumor location, depth of invasion, and other factors. Advanced gastric cancer has a higher incidence of No. 1 LNM. Because upper gastric cancer always occurs in the lesser curvature, and the distance between the No. 1 LNs and the tumor is close, No. 1 LNM is the most frequent in advanced upper gastric cancer, demonstrating an incidence of between 50.0 % and 76.0 % [1–5]. The metastatic rate varies between 14.0 % and 24.0 % in gastric body cancer and between 6.0 % and 18.6 % in distal gastric cancer [6, 7]. Even for early proximal gastric cancer, the incidence of No. 1 LNM can be as high as 4.4 % [8]. However, the incidence of No. 1 LNM is low in early distal gastric cancer. Liu et al. [7] analyzed the status of LNM in 129 patients with early lower gastric cancer and showed No. 1 LNM; they suggested that No. 1 LNs should not be routinely removed for those patients. Thus, No. 1 LNs should be routinely removed for patients with gastric cancer except those with early lower gastric cancer. In addition, lymphatic vessels around the stomach mainly lie along the left gastric artery (LGA), splenic artery, and hepatic artery and finally drain into the celiac artery (CA). The gastric lesser curvature around the CA is a predilection site of LNM, especially the No. 3 LNs, which have a higher metastatic rate. The frequency of No. 3 LNM varied between 50.5 and 65.8 %, as reported [1, 3, 9]. In addition, the incidence of No. 3 LNM in early lower gastric cancer was up to 9.5 % [10]. No. 3 lymph node dissection is also part of D1 lymphadenectomy according to the 3rd edition of Japanese Gastric Cancer Treatment Guidelines [11]. Therefore, No. 3 LNs should be routinely excised during subtotal or total gastrectomy for early or advanced gastric cancer.
The rate of No. 2 LNM was 24.0–40.0 % in middle or upper gastric cancer, which was lower than No. 1 LNM. Moreover, the incidence of No. 2 LNM was even more reduced for lower third gastric cancer, at less than 1.0 % [3, 12]. Dissection of No. 2 LNs is included in D1 lymphadenectomy during subtotal or total gastrectomy for proximal gastric cancer, as based on the 3rd edition of Japanese Gastric Cancer Treatment Guidelines [11]. Thus, No. 2 LNs should be routinely resected during proximal or total gastrectomy, while this dissection can be omitted when undergoing distal gastrectomy.
In conclusion, gastric cancer, especially middle or upper gastric cancer has a higher incidence of LNM in the cardial area. No. 1 LNs should be routinely removed for patients with gastric cancer except those with early lower gastric cancer. No. 3 LNs should be routinely excised during radical gastrectomy for gastric cancer. No. 2 LNs should be routinely resected during proximal or total gastrectomy, while this dissection can be omitted when undergoing distal gastrectomy.
7.2 Anatomy Associated with Lymph Node Dissection in the Cardial Area
7.2.1 Fascia and Intrafascial Space in the Cardial Area
7.2.1.1 Gastrophrenic Ligament (GPL)
The GPL is formed by the cranial part of the dorsal mesogastrium (DM) that extends upward to the diaphragm, and it is continuous with the upper portion of the gastrosplenic ligament (GSL) and the splenorenal ligament (SRL). It is a peritoneal fold between the gastric fundus (close to the cardia) and the left crus of the diaphragm. The fundic branch of the left inferior phrenic artery (LIPA) and the posterior gastric arteries (PGAs) run into the gastric fundus through the GPL (Figs. 7.2, 7.3 and 7.4).
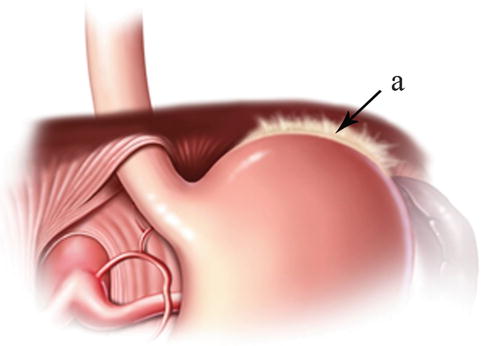
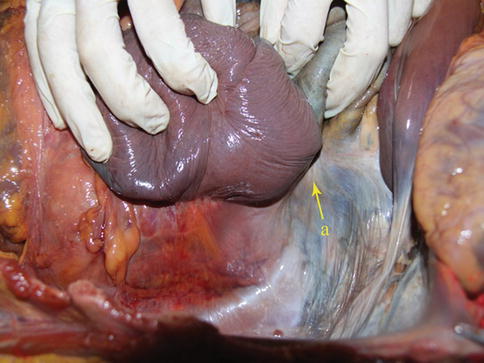
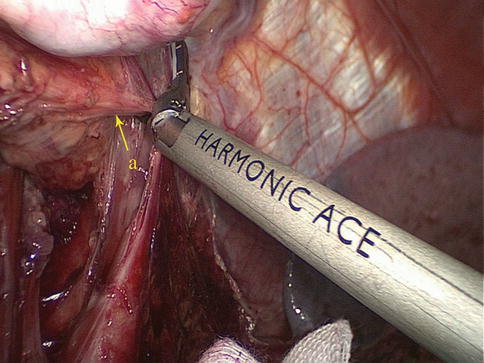
Fig. 7.2
The anterior aspect of the GSL (a)
Fig. 7.3
GSL (a) (In autopsy)
Fig. 7.4
GSL (a)
7.2.1.2 Hepatogastric Ligament
The hepatogastric ligament (HGL) is derived from the primitive ventral mesogastrium, and it extends from the diaphragm and the fossa for the ductus venosus toward the lower left side up to the abdominal esophagus and the gastric lesser curvature (Figs. 7.5, 7.6, and 7.7). The HGL is continuous with the hepatoduodenal ligament (HDL). The HGL carries the right and left gastric vessels running along the gastric lesser curvature as well as the gastric, hepatic, and duodenal branches of the vagus nerve. Variant vessels, such as the left accessory hepatic and gastric arteries, are also included within the HGL.
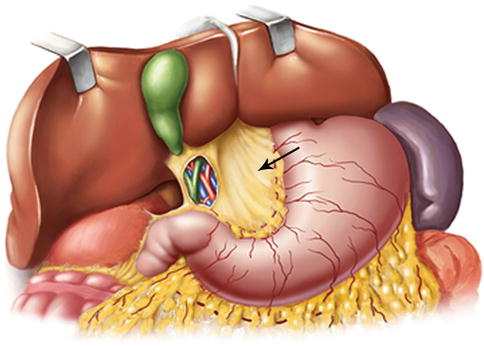

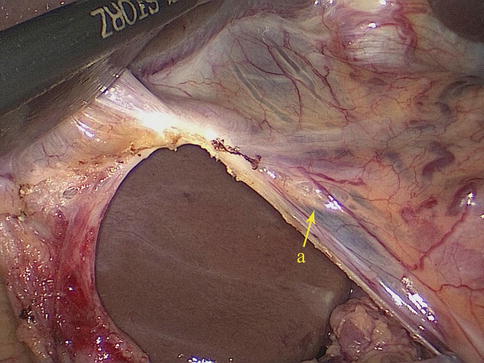
Fig. 7.5
The schematic figure of the HGL (the arrow represents the HGL)
Fig. 7.6
HGL (a) (In autopsy)
Fig. 7.7
HGL (a)
7.2.2 Vascular Anatomy Associated with Lymph Node Dissection in the Cardial Area
7.2.2.1 Arteries Associated with Lymph Node Dissection in the Cardial Area
Terminal Branch of the LGA
After issuing from the CA, the LGA runs toward the upper left side until slightly below the lesser curvature of the cardia, where it enters the HGL. It gives off ascending branches near the gastric wall that join with the esophageal artery. It also branches into two descending gastric branches (anterior and posterior), which run downward and toward the right along the anterior and posterior sides of the gastric lesser curvature. It gives off four to six branches supplying both surfaces of the stomach along the way, and it joins with the right gastric artery (RGA) to form the arterial arch of the lesser curvature (Figs. 7.8, 7.9, 7.10, and 7.11).
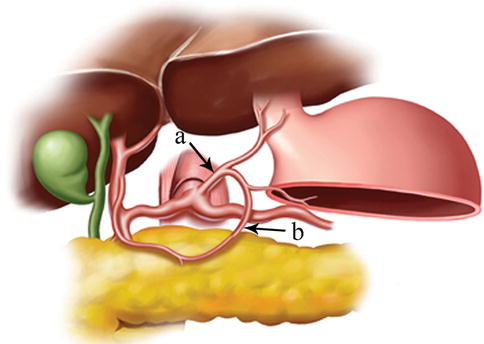

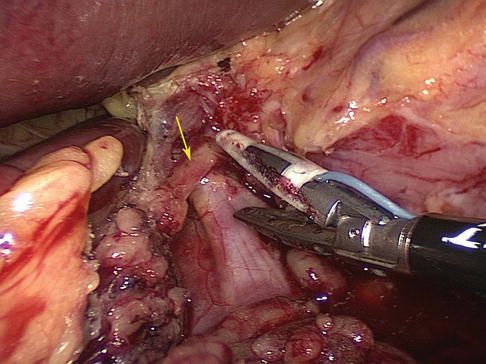
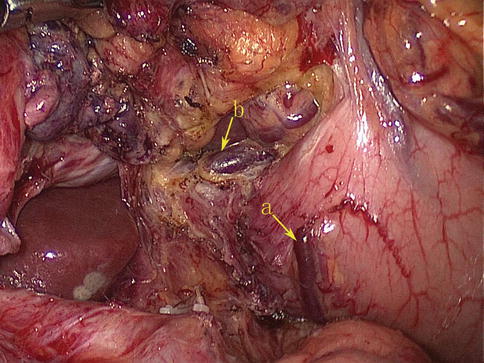
Fig. 7.8
Distribution of the terminal branch of the LGA. The LGA (a). Arterial arch of the lesser curvature (b)
Fig. 7.9
Distribution of the terminal branch of the LGA (a) (In autopsy)
Fig. 7.10
The LGA gives off the ascending branches (the arrow represents the ascending branches)
Fig. 7.11
The LGA sends the anterior (a) and posterior (b) gastric branches
Fundic Branch of the LIPA
The fundic branch of the LIPA is one of the terminal branches of the inferior phrenic artery (IPA), which arises from the abdominal aorta and passes upward to divide into the left and right inferior phrenic arteries. The left passes behind the cardial area and gives off a fundic branch near the gastric fundus, which runs through the GPL to supply the fundus (Figs. 7.12 and 7.13).
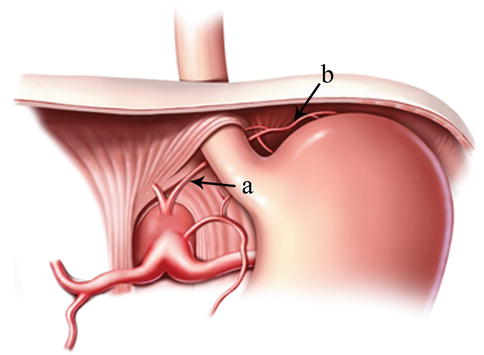

Fig. 7.12
The LIPA (a) gives off the fundic branch (b) to supply the fundus
Fig. 7.13
The LIPA (a) gives off the fundic branch (b) to supply the fundus
7.2.2.2 Veins Associated with Lymph Node Dissection in the Cardial Area
The venous branches from the anterior and posterior walls of the gastric lesser curvature flow in the direction of the cardia within the lesser omentum and join together to form the coronary vein, which then drains into the splenic vein (SV) or the portal vein (PV). The venous branches from the greater curvature of the gastric fundus and cardia form the short gastric veins or the posterior gastric vein (PGV) to end in the SV. Some of the esophageal veins and part of the gastric submucosal venous plexus may join with the esophageal venous plexus to empty into the azygos vein, which communicates with the superior vena cava. This forms the portal-caval venous collateral circulation (Figs. 7.14 and 7.15).

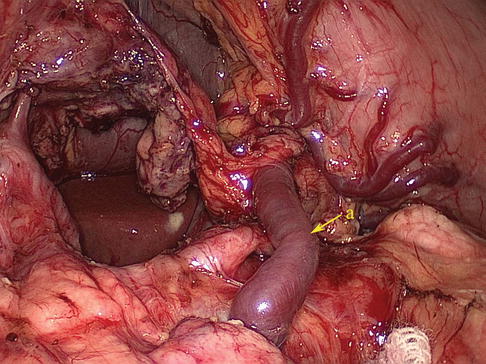
Fig. 7.14
The venous branches from the anterior and posterior walls of the gastric lesser curvature and join together to form the coronary vein (a) (In autopsy)
Fig. 7.15
The venous branches from the anterior and posterior walls of the gastric lesser curvature and join together to form the coronary vein (a)
7.2.3 Lymph Node Anatomy of the Cardial Area
7.2.3.1 The No. 1 LNs (Right Paracardial LNs)
Definition of the No. 1 LNs
The No. 1 LNs are located at the right side of the cardia. They include the LNs lying above the first branch of the ascending LGA (cardial branch) that feeds the gastric walls and those located right at this vessel. This vessel separates the No. 1 LNs from the No. 3 LNs, which lie below it (Figs. 7.16 and 7.17).
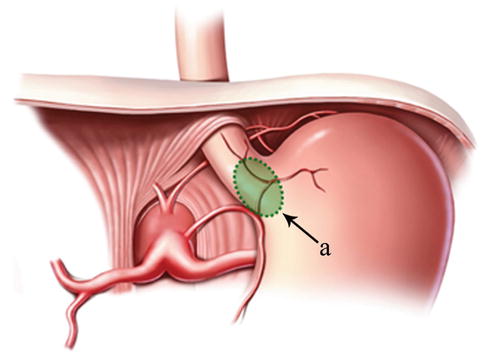
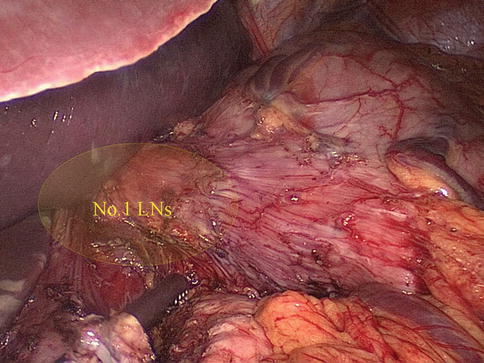
Fig. 7.16
The scope of the No. 1 LNs (a)
Fig. 7.17
The scope of the No. 1 LNs
Case of No. 1 LNM (Figs. 7.18 and 7.19)
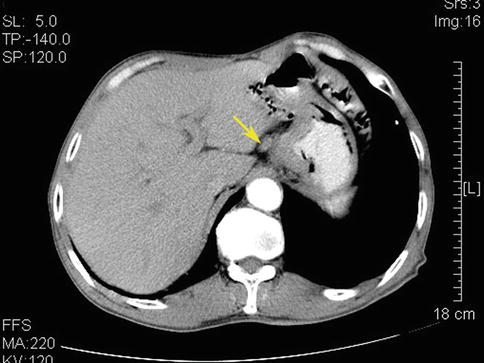
Fig. 7.18
CT scan showing No. 1 LNM (the arrow represents the swollen No. 1 LNs)
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:
 The Current Status and Development of Lymph Node Dissection for Gastric Cancer
Summary of Anatomy and Physiology of Perigastric Lymphatic System
Prevention and Treatment of Complications Associated with Laparoscopic Surgery for Gastric Cancer
The Current Status and Development of Lymph Node Dissection for Gastric Cancer
Summary of Anatomy and Physiology of Perigastric Lymphatic System
Prevention and Treatment of Complications Associated with Laparoscopic Surgery for Gastric Cancer
 Preoperative Notes of Laparoscopic Lymph Node Dissection for Gastric Cancer
Preoperative Notes of Laparoscopic Lymph Node Dissection for Gastric Cancer
 Laparoscopic Infrapyloric Area Lymph Node Dissection for Gastric Cancer
Laparoscopic Infrapyloric Area Lymph Node Dissection for Gastric Cancer
 Laparoscopic Suprapancreatic Area Lymph Node Dissection for Gastric Cancer
Laparoscopic Suprapancreatic Area Lymph Node Dissection for Gastric Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


