with hiatal hernia, which tends to promote free gastroesophageal reflux, as the additional safety valve of the diaphragmatic pinch is less effective. Other patients have motility problems that allow reflux of gastric contents into the esophagus or have a degree of peristaltic failure.
Table 10-1 Classification of Esophagitis by Etiology | |||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||
along with increased transient LES relaxations (tLESR) cause reflux disease. Besides increased relaxation, or insufficiency of the distal esophageal sphincter, there are other factors that can either cause or unmask prior existing reflux disease. These include the presence of a hiatal hernia (Fig. 10-1), the increased acid secretion that often follows H. pylori eradication therapy (or rarely Zollinger-Ellison syndrome), obesity, medications that decrease the LES pressure,9 possibly excess alcohol, impairments of esophageal emptying (motility disorders), impaired salivary and esophageal gland secretions, duodenogastric reflux, delayed gastric emptying (mostly in diabetic patients with autonomic neuropathy), stenosis or strictures, impaired esophageal resistance to acid, and failure of clearance. Numerous changes occur in the esophageal nerves (described under morphologic changes in nerves).
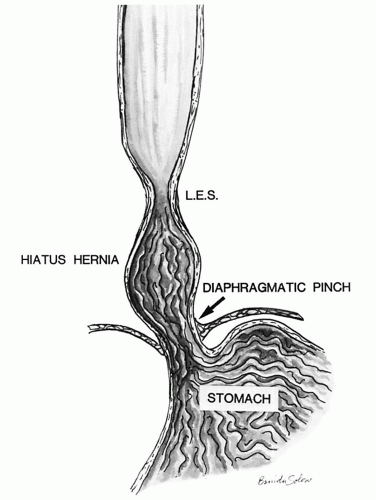 Figure 10-1. Sketch of a sliding hiatus hernia. The LES is located in the chest above the diaphragm. (Courtesy of E. Hassall, MD.) |
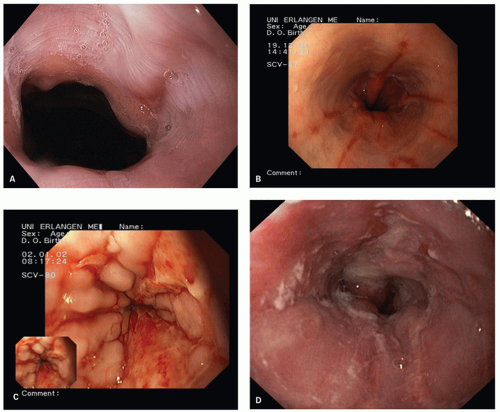 Figure 10-2. Reflux esophagitis: Endoscopic appearance of Los Angeles A-D reflux esophagitis. (Courtesy of Steffen Muehldorfer, MD.) A: Grade A: A mucosal break <5 mm long between the tops of the mucosal folds at the right side of the esophageal wall. B: Grade B: Six mucosal breaks more than 5 mm long between the tops of the mucosal folds. C: Grade C: Mucosal breaks that extend between the tops of two or more mucosal folds, but involve <75% of the esophageal circumference. D: Grade D: Mucosal breaks that involve more than 75% of the esophageal circumference. |
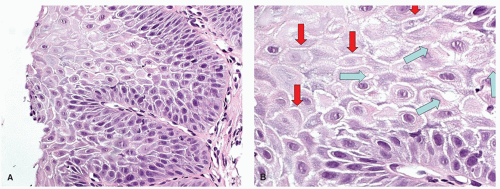 Figure 10-3. Dilated intercellular spaces. A: Overview of an esophageal biopsy with overt basal cell hyperplasia. DIS tends to be maximal around the papillae. B: Detail showing DIS that can take the form of exaggerated intercellular prickles (ladders) between any two cells (red arrows), or “bubbles” at the junctions of three cells (blue arrows). |
is that of red streaks of the distal esophagus. These are covered by a thin layer of newly re-epithelialized squamous epithelium with underlying capillary-rich granulation tissue.21 Frequently, such lesions can be seen after healing of erosions (mucosal breaks).
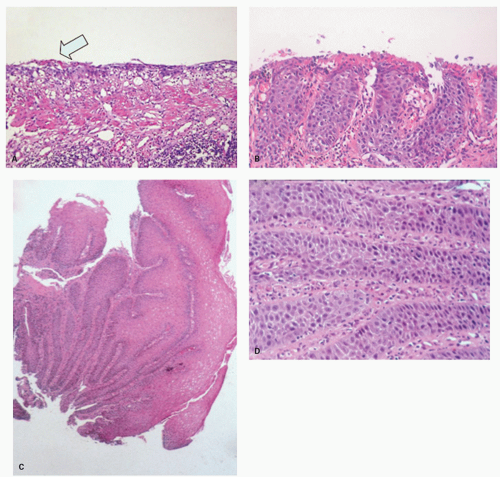 Figure 10-4. Erosions and sequela. A: Erosion with a wisp of superficial restituting epithelium (left arrow). Lesions such as these can be seen when red streaks seen endoscopically are biopsied. B: Erosion undergoing re-epithelialization. The epithelium consists entirely of basal cells dipping into the underlying granulation tissue. C-E: Healing erosion with marked pseudoepitheliomatous hyperplasia. The distinction from neoplasia at low power is the regularity of the “prongs.” |
neutrophils that are initially superficial (Fig. 10-5), and a sprinkling of eosinophils (Fig. 10-5) that are less than those seen in EoE (<25 in 1 high-power field [HPF] or 15 in each of 2 in the same biopsy, and usually far fewer than this) but are usually sufficiently uncommon that one usually has to search for them. There is an overlap with EoE (see that section); patients with typical clinical, endoscopic, and histologic features of EoE are usually treated as such but where these are not all present (and in some patients with typical features of EoE), they are often treated for GERD, at least initially. A rare eosinophil is thought to be acceptable in adults, although they remain uncommon, but in children eosinophils are always regarded as abnormal. An excess of intraepithelial lymphocytes (IELs) (lymphocytic esophagitis) is seen in GERD but appears
to be neither sensitive nor specific; nor has the cut-off for normals been well defined. As such, this cannot reasonably be used to make a diagnosis of GERD.
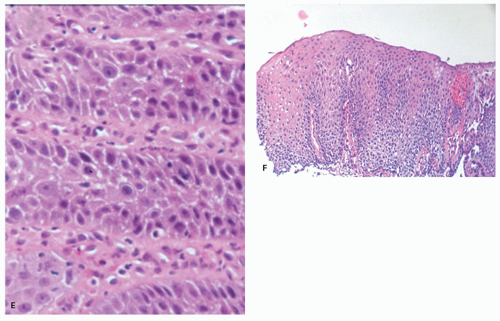 Figure 10-4. (Continued) F: More typical reactive changes in which the acanthotic epithelium has basal cell hyperplasia and papillae extend about 80% of the way to the surface. To the right there is a hemorrhagic papilla and the remnants of granulation tissue. |
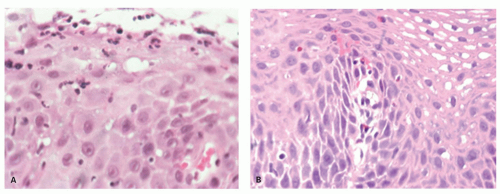 Figure 10-5. GERD. A: (detail C) Esophageal mucosa with superficial neutrophils. While this can be seen in GERD, it can also be part of drug-induced injury and infections such as Candida. |
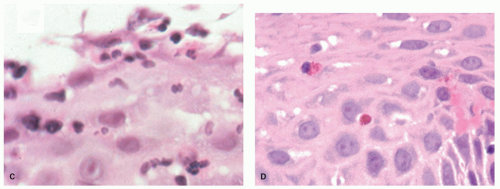 Figure 10-5. (Continued) B: (detail D) Epithelium with scattered eosinophils indicative of GERD. |
gastric intestinal metaplasia, or limited to the cardia, and be GERD related.
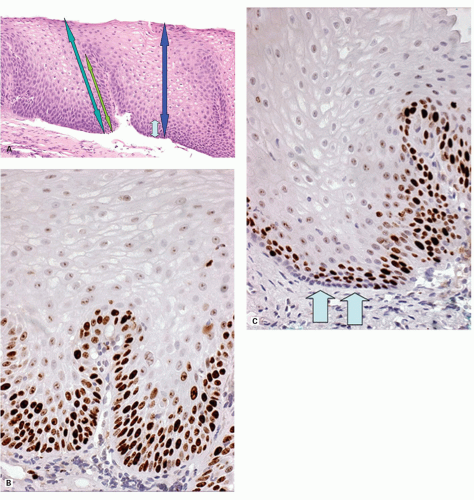 Figure 10-6. Reactive changes in squamous mucosa. A: Normal squamous epithelium with small layer of basal cells extending about one-sixth of the distance to the surface (light blue and dark blue arrows right). The epithelial papillae do not extend more than about two-thirds of the entire epithelial thickness. This can be gauged by dividing the epithelium into thirds (light green and dark green arrows left). The papillae should not extend into the upper one-third, while if the basal third is mentally divided into thirds, the basal layer should not occupy more the half of this. The basal layer stops where the distance between nuclei is greater than the nuclear diameter. B,C: Ki-67 immunostain in reactive hyperplasia (B) and normal mucosa (C). In normal mucosa (right) the proliferative zone is above the most basal layer (arrows) suggesting that the nonproliferating cells are “stem cells.” In reactive changes (left) they are all reincorporated into the proliferative zone. |
Table 10-2. Reflux-independent Esophageal Lesions | |||||||||
|---|---|---|---|---|---|---|---|---|---|
|
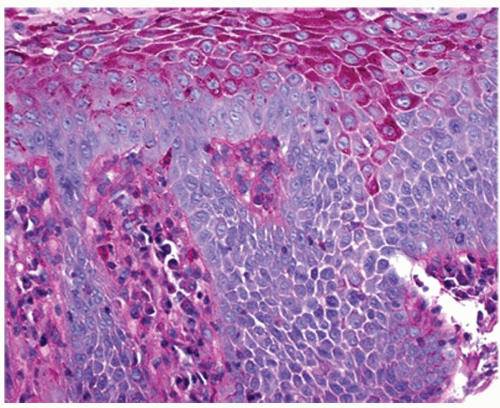 Figure 10-7. PAS stain showing PAS-positive glycogen-containing cells that are not present in the basal cells and are limited to the nonbasal superficial cells. |
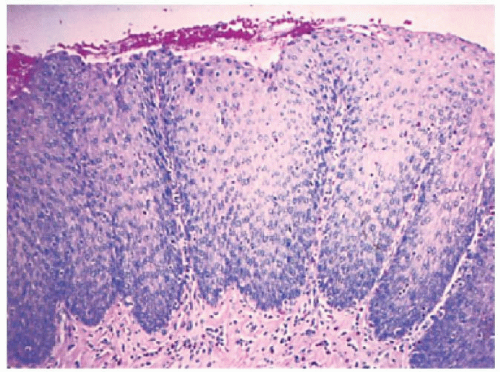 Figure 10-8. The dermal papillae are elongated, and the basal cell zone is expanded to more than 15% of the squamous layer’s thickness. If these changes were found in a biopsy that included the Z-line, or were stated as being within 3 cm of the Z-line, it is appropriate to say that “reactive changes are present but in this location they may be physiologic.” |
In practice, the most relevant (specific) criteria are thickness of the basal cell layer (>15%) and proportional length of papillae (>2/3),26, 27, 28 the latter invariably coming out as the best criteria in clinical studies. This may be useful as it suggests that the presence of an erosion or ulcer without immediately adjacent reactive changes in the squamous mucosa may be an indicator of acute damage (pills) rather than more chronic intermittent disease (reflux).
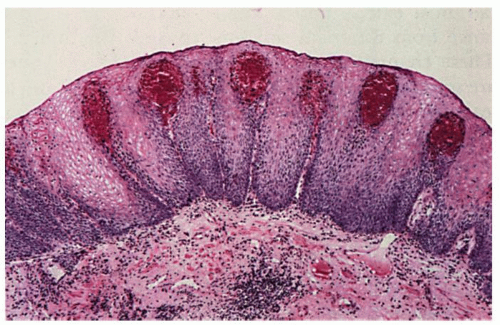 Figure 10-9. Dilated vessels in papillae (vascular “lakes”). |
(Fig. 10-10), so it is usually assessed more precisely endoscopically.
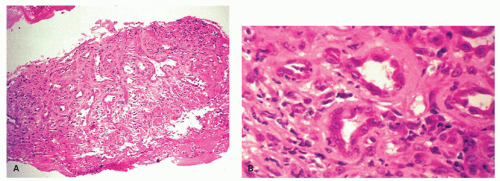 Figure 10-10. Exuberant granulation tissue in ulcerative esophagitis can mimic adenocarcinoma. A: Low-power view of a biopsy specimen from an esophageal ulcer. B: High-power view shows the microvessels of the granulation tissue. |
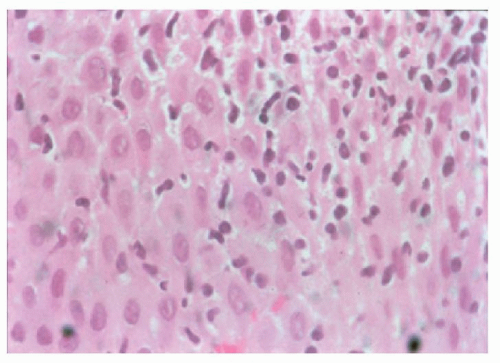 Figure 10-11. Esophageal mucosa with myriad IEMs, most of which are lymphocytes, but antigen-presenting cells and sometimes mast cells may all be present. |
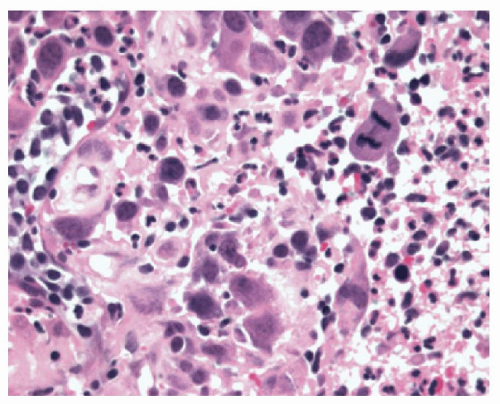 Figure 10-12. Reactive (pseudosarcomatous) changes in the stroma. Note the lack of cohesion, large nuclei but with indistinct chromatin, and, in this example, mitotic figures. These cells are immunoreactive to vimentin, sometimes CD10, and occasionally Ki-67. |
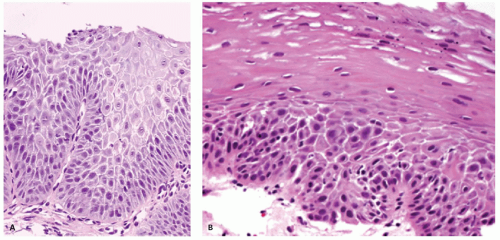 Figure 10-13. Reactive hyperplasia (A) versus low-grade squamous dysplasia (B). Note the orderly maturation in the squamous mucosa but disorderly maturation, sometimes with almost an abrupt transition from immature to mature epithelium as shown here. A helpful clue is that other features of reactive changes (papillary hyperplasia, extensive dilatation of intercellular spaces) are present on the left, but rarely present in squamous mucosa. Although dilated intercellular spaces are present in the dysplastic mucosa on the right, they stop abruptly where the squamous dysplasia stops. |
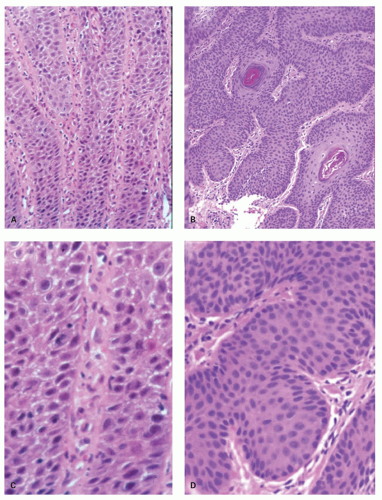 Figure 10-14. Reactive versus neoplasia. The panels on the left (A,C) show orderly reactive hyperplasia where the squamous rete pegs (prongs) are orderly and predictable in their regularity. In comparison, in this example of one of the best-differentiated squamous carcinomas we could find (B,D), the major difference is at low power (A,B) where the tumor grows in a disorderly and unpredictable manner. The details (C,D) show dysplastic mucosa to primarily have greater cellularity. Loss of polarity, especially in the basal layer, together with lack of reproducibility between adjacent cells, and greater hyperchromatism in dysplastic mucosa tend to be the best features. |
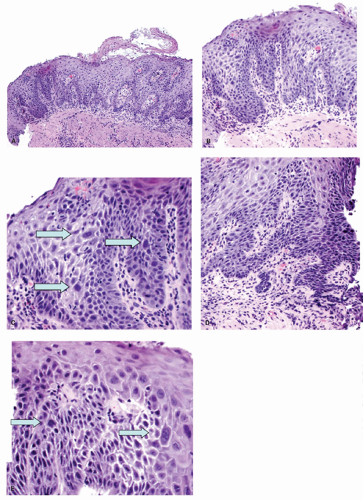 Figure 10-15. Atypia in squamous mucosa. A: Overview of lower esophageal biopsy showing marked nuclear changes, especially in the papillae that extend very close to the surface. Note that the epithelium rests almost on top of the muscularis mucosae with virtually no lamina propria, suggesting that this is a re-epithelialized erosion. B,C: Details of the left end of (A), with enlarged atypical nuclei (arrows). D,E: Adjacent field from (A) showing the restituting edge of an erosion lower right (E), immediately adjacent mucosa to (D), with further individual atypical cells, the largest (right) in E being binucleate (arrows). Situations such as these are best handled by treating with PPIs and repeating the biopsies within a month or two. Endoscopy should be carried out with high a resolution endoscope, biopsies being directed at atypical areas. |
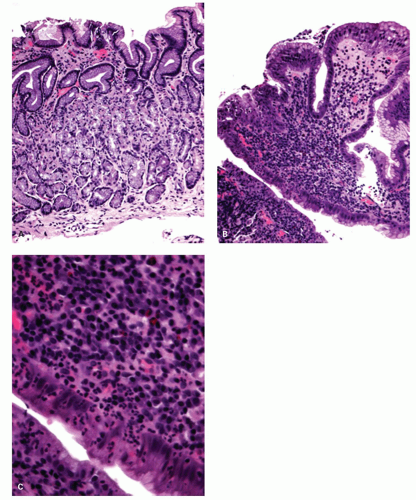 Figure 10-16. Chronic active carditis. A: Antral biopsy with no hint of Helicobacter gastritis (key in determining that this is the case, as antral and cardiac mucosa tend to resemble each other in Helicobacter infection). B: Biopsy from cardia— same patient and same magnification as “A” showing marked inflammation. C: Detail of (B) showing the chronic active inflammation. In the differential diagnosis, the severe chronic inflammation makes medication use unlikely and Crohn’s disease is unlikely as a presenting manifestation. This essentially leaves GERD or an “idiopathic” etiology. The former seems the most likely choice. Diagnosis was “chronic active carditis that, in the absence of Helicobacter, is most likely GERD-related.” |
development of carcinoma is 40- to 125-fold higher in BE compared to in the normal population (see following Section and Chapter).
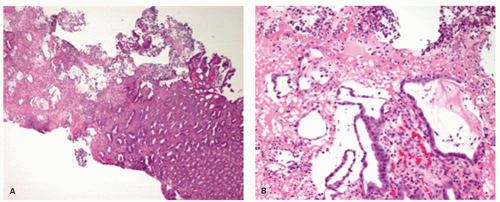 Figure 10-17. Cameron’s ulcer in a hiatal hernia. A: Oxyntic mucosa (right) with an exudate on the surface (left). B: Detail of part of the pseudomembrane showing pits with attenuated restituting epithelium in a fibrin neutrophil exudate and bearing considerable resemblance to pseudomembranous colitis. Although no fibrin thrombi are present in this biopsy, its apparent acute ischemic nature is apparent. |
that goblet cells are lurking in there somewhere and just need to be found.
recognition of the diaphragmatic pinch can also be useful, especially in establishing the presence of a hiatal hernia that invariably accompanies BE (Fig. 10-18), but when the squamous mucosa is inflamed it becomes red, so the proximal limit of the Z-line may not be apparent, and it is here that biopsies may be required to confirm that the proximal mucosa is indeed columnar and not squamous. The top of the gastric folds marks the proximal limit of the stomach (Fig. 10-19), although this is not as easy as it seems, as it depends in part on the degree of insufflation.
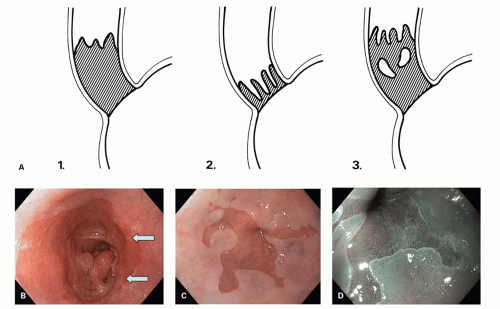 Figure 10-18. Endoscopic appearances of BE. A: Sketch illustrating the patterns. A common pattern is shown in panel 1. The interface between the Barrett’s (hatched) and squamous mucosa is often wavy, as shown, similar to the Z-line at the GEJ. Panel 2: Short segment with tongues only, that is, no circumferential involvement. Panel 3: Residual whitish squamous islands are commonly present, especially near the upper end of Barrett’s mucosa. B: Endoscopic view of long-segment Barrett’s with circular columnar metaplasia and small islands of squamous epithelium (arrows). C: Tongues of columnar metaplasia in the distal esophagus (BE) in white light. D: NBI technique with regular gyriform surface epithelium pattern. (Images courtesy of Steffen Muehldorfer, MD.) |
this is that it is impossible to make a confident diagnosis of BE until the proximal extension of columnar mucosa, whether a tongue or circumferential extension, is at least 1 cm in length. Less than this it is simply an irregular Z-line by definition. The corollary of this is that it is impossible to separate “ultra-short” BE (<1 cm of BE) from intestinal metaplasia in native cardiac mucosa. Although ultrashort BE presumably must exist, at the time of writing there is no good way to make that diagnosis by biopsy of this region alone. If intestinal metaplasia is isolated to the cardia region without the rest of the stomach being involved, this implies that it may well be GERD related and therefore Barrett’s related, but this remains implied and not definitive. The latter requires biopsies of that area most likely to have intestinal metaplasia, namely, the antrum and incisura region of the stomach, the most likely cause of which is Helicobacter, and which is mirrored at the cardia. If biopsies are carried out to ascertain this, those from the cardia must necessarily be placed into a separate container to allow identification of cardiac and antral pathology separately.
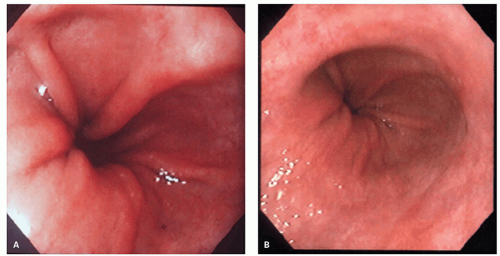 Figure 10-19. Endoscopic Landmarks: Recognizing the GEJ. A: Top of the gastric folds. B: LES pinch that is frequently lax in patients with GERD-associated disorders. Here it is at the top of the gastric folds. |
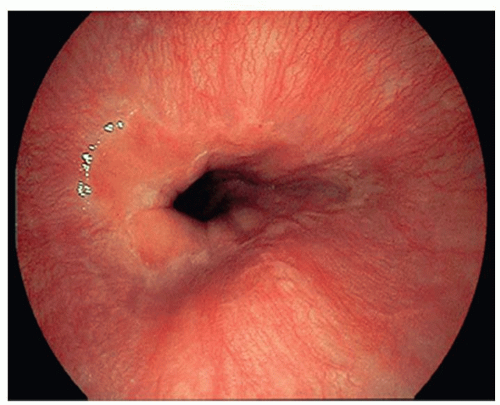 Figure 10-20. Endoscopic landmarks of the distal end of the esophagus (in Japan) showing the limits of the palisaded vessels. In this example, they focally descend beyond the upper limit of the gastric folds. |
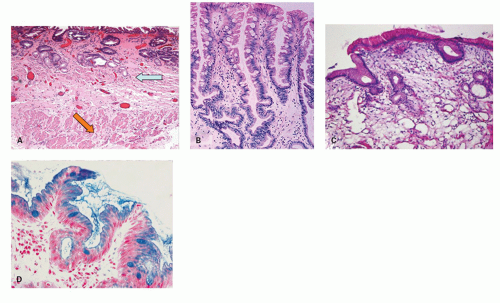 Figure 10-21. A: Histology of columnar metaplasia with goblet cells/specialized intestinal metaplasia and double muscularis mucosae. The marked and diffuse intestinalization in the lower esophagus is virtually diagnostic of BE as such metaplasia is only seen in gastric mucosa with diffuse intestinal metaplasia. In addition, the duplicated muscularis mucosae is clearly visible with a superficial (neo) layer immediately beneath the epithelium (blue arrow) and the original muscularis mucosae beneath (orange arrow). Courtesy of Dr. C Streutker. B: Typical biopsy appearances of BE with incomplete intestinal metaplasia and branching pits. C: Histology of columnar metaplasia without goblet cells. This patient had a 3.5-cm circular segment of columnar metaplasia in the distal esophagus with no significant hiatal hernia. Repeated endoscopy and multiple biopsies still did not show goblet cells. D: Alcian blue stain at pH 2.5. While the goblet cells stain, many of the intervening columnar cells also stain. Not only can interpretation be difficult but it can sometimes be positively misleading. We rarely carry out this stain for diagnostic purposes. |
metaplasia at index endoscopy showed intestinal metaplasia after 5 years, while at 10 years the figure reached 91%. Thus, 9% of patients in these cohorts never had goblet cells detected over that time period.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


