Table 18-1 Normal Colonoscopy and Abnormal Histology | ||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||
other forms of colitis have been described,19, 20, 21, 22, 23, 24 some of which are variants of these two disorders, while others appear to be distinct nosological entities.25, 26, 27, 28, 29, 30 However, in current practice the use of the term “microscopic colitis” largely implies either collagenous or lymphocytic colitis and their variants, and the other conditions like eosinophilic colitis or possibly mastocytic enteropathy are designated by their specific names.
Table 18-2 Medications Potentially Related to the Development of Lymphocytic Colitis | |
|---|---|
|
Table 18-3 Autoimmune Disorders Associated with Microscopic Colitis | ||
|---|---|---|
|
Reduced matrix degradation is supported by the reduced expression of the collagenase matrix-metalloproteinase (MMP)-1 and increased expression of tissue inhibitor of metalloproteinase-1 (TIMP-1).65 A rare case of collagenous colitis associated with osteogenesis imperfecta, which is an inherited disorder of collagen synthesis has also been reported.66 Decreased expression of occludins and claudin-4 has been shown in collagenous colitis suggesting defects of epithelial barrier function in collagenous colitis.64 Increased expression of TGF-β1 in eosinophils, cyclooxygenase-2 (COX-2) in macrophages, connective tissue growth factor (CTGF) in myofibroblasts, mucosal basic fibroblast growth factor (bFGF), increased mucosal expression of vascular endothelial growth factor (VEGF), and increased endoluminal nitric oxide have all been reported in collagenous colitis.67, 68, 69, 70, 71 A reduced expression of CD1d has been shown in colonic epithelium of patients with microscopic colitis.72 CD1d is a major histocompatibility complex class I—like molecule, which is involved in regulating normal immunity of the gastrointestinal tract (GI) and thus disordered mucosal immunity may play a role in the pathogenesis. Active collagenous colitis is also associated with a TH1 and interferonγ mucosal cytokine profile, similar to patterns found in celiac disease.73 Number of eosinophils and mast cells are increased in microscopic colitis. Eosinophil activation may affect mucosal permeability.74, 75 Also, increased production of histamine by mast cells may promote diarrhea.76
(up to 70). One needs to be careful when interpreting a tangential section, where the basement membrane may artifactually appear thicker (Fig. 18-3A).
Table 18-4 Comparison of Collagenous and Lymphocytic Colitis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
collagen layer may be patchy, both within a biopsy specimen as well as between specimens from different regions of the colon, usually being thickest in the transverse colon. Thickening increases toward the right side of the colon and can be absent in the sigmoid colon and rectum. The rectum is spared in approximately 30% to 40% of cases.85, 86 Thus, rectal biopsies alone may miss this disease. While initial workup of patients (with flexible sigmoidoscopy) to rule out microscopic colitis with four biopsies every 10 cm from the left colon may be appropriate, negative results should be followed up with a full colonoscopy.87 Also, initial evaluation may miss the diagnosis in a good number of cases (one fourth to one third), which may either be related to sampling or lack of fully developed histology at the time; hence, there is a role for repeat colonoscopy.31, 88
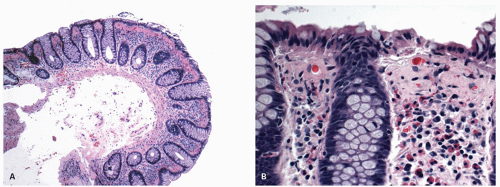 Figure 18-1. Collagenous colitis. A: Low-power view of an obvious example of collagenous colitis. Overview shows crypts with a normal architecture which may not extend as close to the muscularis mucosae as usual. The subepithelial collagen band, which occupies the upper quarter of the mucosa and measures about 60 µm in thickness, is apparent. B: High power: The luminal epithelium may be normal, but is often injured and cuboidal or low columnar with intraepithelial inflammatory cells. The inflammatory cells are mainly lymphocytes and are frequently very prominent. However, eosinophils and less frequently, neutrophils can be present. Also note the capillaries entrapped in the thick collagen layer; sometimes, when the thickness of the band is equivocal this feature may support a diagnosis of collagenous colitis. |
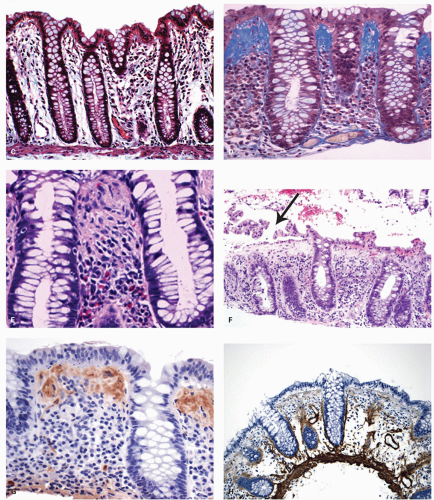 Figure 18-1. (Continued) C: Trichrome stain showing normal subepithelial and pericryptal collagen, as compared with markedly thickened subepithelial collagen in an example of collagenous colitis in (D). E: Sometimes, the eosinophils can be very prominent in the inflammatory infiltrate. F: Collagenous colitis with stripping of the surface epithelium (arrow). This is sufficiently characteristic of the disease that its presence should prompt immediate examination of the underlying collagen band, which here is greatly thickened. G: Immunostain for laminin shows strong positivity in the thickened subepithelial collagen, while staining for collagen type IV (basement membrane collagen) is negative (H). |
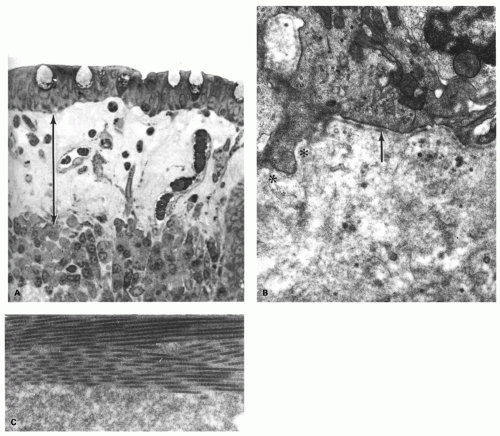 Figure 18-2. A: Electron micrograph of the subepithelial collagen layer. One mircometer epon section showing the thick subepithelial band and characteristic trapped capillaries underneath the epithelium. B: The basement membrane region (arrow) in collagenous colitis is commonly deficient focally (asterisk). The collagen layer itself consists of a mixture of amorphous ground substance and mature collagen. C: Detail to show the interface between the collagen fibers above and the ground substance below. (B and C, Courtesy of Dr. T.K. Shnitka.) |
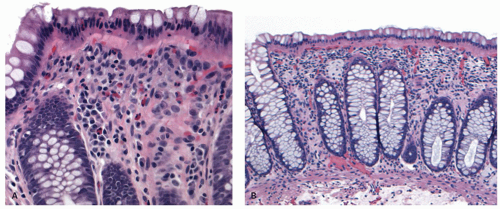 Figure 18-3. Possible errors in diagnosis. A: Tangential sectioning; the underlying crypts are visible in cross section, causing an artifactual impression of thickening of the collagen band. B: Nuclei of luminal epithelium are in the center of the cell, so that an eosinophilic zone is present beneath them, which can be mistaken for a thickened collagen band. |
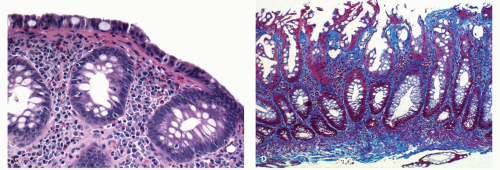 Figure 18-3. (Continued) C: Thickening of the subepithelial collagen that is <10 µm. Compare with the adjacent nuclei of lymphocytes. In the presence of increased IEL, lamina propria infiltrate, and epithelial injury, it certainly represents microscopic colitis, and a diagnosis of lymphocytic colitis would be favored. D: Marked thickening of subepithelial collagen in a hyperplastic polyp. Remaining colonic mucosa in this fragment and other colonic biopsies from this patient do not show any evidence of collagenous colitis. |
distortion should lead to a suspicion of IBD, and in the presence of normal endoscopy, this has been referred to as “minimal change colitis” (see later), which usually behaves as ulcerative colitis (UC).12 Paneth cell metaplasia is not uncommon and is seen more frequently with collagenous colitis than lymphocytic colitis.93 Paneth cell metaplasia has been noted more frequently in patients whose symptoms like abdominal pain are ongoing or recurrent, and it was suggested that its presence may be used as a marker to predict more persistent or severe disease.93, 94 Some patients who have patchy thickening of subepithelial collagen layer may show some biopsies with typical features of collagenous colitis, while others resemble lymphocytic colitis, possibly accounting for cases reported in the literature with combined lymphocytic colitis and collagenous colitis.43 When there is evidence of both conditions (i.e., lymphocytic colitis with a thickened subepithelial collagen band), collagenous colitis “trumps” lymphocytic colitis by convention. Some patients with lymphocytic or collagenous colitis have extensive involvement of the GI tract including stomach and small bowel (pan gastroenterocolitis) (see also collagenous gastroenterocolitis).95, 96
should be seen in just more than one well-oriented biopsy fragment and is a useful diagnostic feature appreciated even at low magnification.24 When inflammation is marked, plasma cells may reach the muscularis mucosae thereby mimicking IBD. A variety of other cells may also be increased in numbers, including neutrophils and eosinophils (Fig. 18-4A-C). Cryptitis when seen is usually focal.93 The crypt architecture is generally well preserved and minimal crypt distortion with an occasional bifid crypt can be seen (Fig. 18-4C).93 Paneth cell metaplasia may also be seen. Usually, the disease tends to be diffuse throughout the large bowel and the rectum is spared in about 8% of cases.120 Random rectal biopsies are therefore likely to provide false-negative biopsies, while biopsies from the more proximal left colon in addition (descending and sigmoid colon) markedly increase the chances of getting the correct diagnosis.
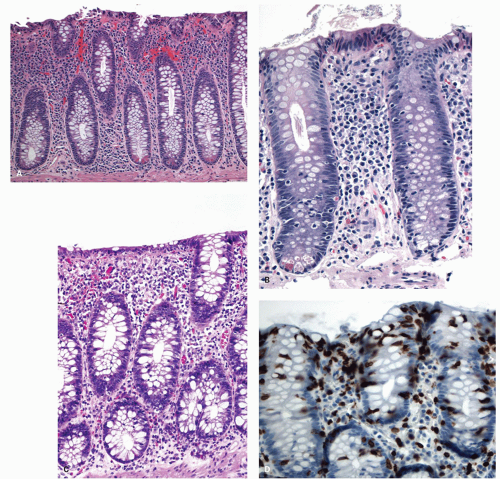 Figure 18-4. Lymphocytic colitis. A,B: The architecture is intact, with evenly spaced crypts pushed apart by an inflammatory infiltrate. Surface epithelial cells are often cuboidal but can be tall and columnar. Numerous IEL are present. The subepithelial collagen band approximates the thickness of the diameter of the adjacent lymphocyte or plasma cell nuclei, and therefore is within the normal range although it can be slightly thickened. C: Occasional crypt branching is acceptable for the diagnosis of lymphocytic colitis. D: Staining with antibodies against CD3 confirms and illustrates more clearly the presence of numerous intraepithelial T cells; however, one seldom needs the stain to make the diagnosis. |
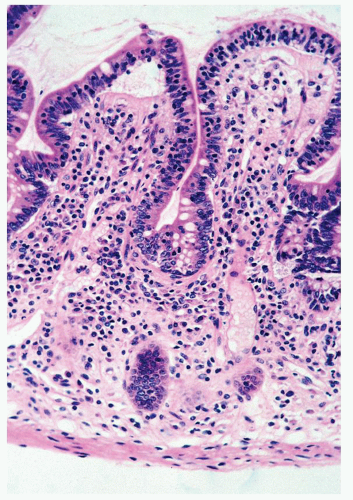 Figure 18-5. Lymphocytic colitis can be associated with lymphocytic ileitis characterized by regular flattening of villi, cuboidal surface epithelial cells, and an increase of IEL. |
Although patients respond to medical therapy, relapses are frequent after stopping the medication. If the initial therapy fails, treatment with steroids or even more potent immunosuppressives can be used. Some patients appear refractory to all therapies and rarely colectomy may be considered. Fecal diversion is also reserved for extremely resistant cases, but is seldom required.43
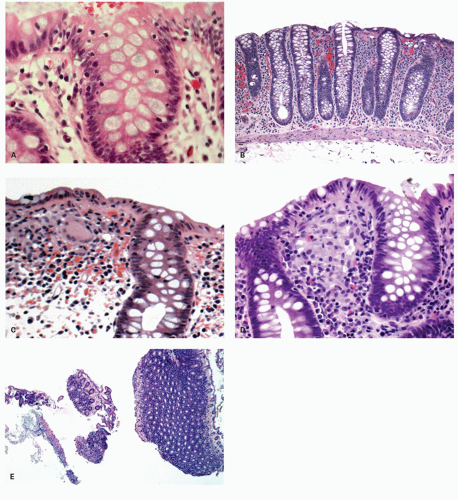 Figure 18-6. A: Variants of lymphocytic colitis characterized by increased IEL, but lacking a dense lamina propria infiltrate of lymphoplasmacytic infiltrate. B: Another example of patient with clinical profile typical for lymphocytic colitis, but the mucosal biopsy showing only increased lamina propria lymphoplasmacytic infiltrate without increase in the IEL. C: Another variant of “microscopic colitis” characterized by the presence of numerous giant cells in the subepithelial location that has been called “giant cell colitis.” D: Granulomatous variant of microscopic colitis with poorly formed granulomas/large collections of histiocytes that were diffuse throughout the superficial lamina propria, remaining features being those of microscopic colitis. E: Occasionally, biopsies show a thickening of the subepithelial collagen band in one sample as illustrated here in a low-power view, and band of inflammatory exudate. This combination may be due to a “pseudomembranous variant” of “microscopic colitis.” |
(Fig. 18-6A,B).127, 128 In addition, while most of these patients have a typical lamina propria lymphoplasmacytosis, some of these may have either patchy involvement or minimal to no increase in IELs (Fig. 18-6B),127, 128 in which case the distinction from normal or Brainerdtype diarrheas can be tricky. These patients seem to have similar clinicopathologic associations as classic lymphocytic colitis patients.22, 128 However, another study showed a different result suggesting paucicellular lymphocytic colitis does not behave like lymphocytic colitis,127 but that unlike most patients with typical collagenous colitis or lymphocytic colitis who have numerous CD25+ FoxP3+ (T-reg) cells in the lamina propria, these patients appear to lack them.127 The low number of IEL can be explained in some patients by a response to symptomatic treatment.
Youngest child reported with collagenous colitis has been of 9 months of age, where collagenous colitis was associated with collagenous gastritis and collagenous spruce with no response to gluten-free diet.133 In general, children have more frequently concomitant collagenous gastritis, duodenitis, and other systemic autoimmune disorders including celiac disease and immunodeficiency syndromes.134, 135 Association with autism, H. pylori, and medications have also been reported.49 Response to treatment is variable and long-term outcome of microscopic colitis in children remains unclear.
and an increased risk for IBD. This association has been substantiated by the results from studies in the United States, Sweden, United Kingdom, and South Africa. The results from incidence studies in Israel however are not so different from those obtained in other high-incidence areas such as the United Kingdom and Scandinavia. In the past, IBD was thought to be more common in whites than in blacks. In Cape Town, South Africa, incidence rates between 1980 and 1984 were eight times higher for whites for UC. Changes in trend have however been observed over the years and now it appears that incidence rates in blacks may actually be closer to those in Caucasians.152, 153
genetic factors may have a more dominant role in CD than in UC. The rate of concordance for CD has been reported to be 30.3% in monozygotic twins and 3.6% in dizygotic twins.170 When identical twins with CD have both IBD, the disease appears to be remarkably similar.171 With UC, the reported concordance rates are 15.4% for monozygotic twins and 3.9% for dizygotic twins.170 Significantly higher concordance rates in monozygotic twins for CD compared to UC suggest that genetic factors probably play a larger role in CD compared to UC.
separately to one disease or the other. For example, they can involve intracellular (NOD2) or cell surface (TLR) bacterial recognition, antigen processing (HLA molecules), or a breakdown in epithelial integrity (DLG5—Drosophila Discs Large Homolog).179 New loci for UC include genes implicated in mucosal barrier function (ECM1, CDH1, HNF4α, and laminin B1); further, E-cadherin is the first genetic correlation between colorectal cancer (CRC) and UC. Impaired IL-10 signaling also seems to be a key pathway in intestinal inflammation.180
Table 18-5 Genomic Regions Significantly Associated with IBD in Genome-wide Association Studies of Patients of European Ancestry | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
enterovirulent E. coli—for CD and UC) have been unequivocally identified as etiologic agents, although some may definitely initiate a first attack of IBD.184, 185 A number of groups in North America and Europe have identified a novel E. coli of the B2 and D phylotypes to be associated with CD that have been termed adherent-invasive E. coli.186, 187, 188, 189 Helicobacters have been isolated from human feces and human colon tissue, and in animal models they can cause an IBD-like disease, but on the evidence available, H. pylori does not seem to have a role in the cause of IBD.190, 191, 192, 193
similar work on CD.215, 216 Attempts to identify infective agents in the stool and mucosa or to demonstrate raised antibody titers to particular organisms in patients’ sera are problematic. The difficulty is to establish whether an abnormality, when present, is the primary defect or simply a secondary phenomenon. Patients with UC have raised antibody titers to numerous organisms including a lipopolysaccharide extract of E. coli O14, an antibody common to most Enterobacteria.217, 218 This antibody cross-reacts with goblet cell antigen in colonic epithelium.219 Similar antibodies are found in first-degree female relatives who have an undamaged mucosa.220, 221 The sharing of antigens between the large intestine and intestinal bacteria has also proved the basis of methods for inducing experimental colitis in animals.219, 222 Raised antibody titers have also been demonstrated to certain Bacteroides spp., Eubacterium, Peptococcus, and Mycobacterium kansasii antigens,223, 224 possibly suggesting a leaky mucosa for bacteria and secondary antibody generation. ASCA, ANCA, and similar antibodies may be generated on the same basis.
hypothesis has not been rigorously tested. The concept has however been broadened to include a large range of microparticles ingested, as part of the diet. These particles are taken up by the specialized M cells that cover the lymphoid follicles, especially Peyer’s patches. They are undegradable and accumulate in lymphoid tissue. They may act as adjuvants, permitting the absorption of other antigens and by doing so, alter the immune system.
clinical activity index, with 40% experiencing remission by 12 months. Appendiceal histology in 29 cases demonstrated ulcerative appendicitis, but no patient had any evidence of typical acute appendicitis.260 A randomized control trial of appendectomy as therapy for UC is clearly needed. Many studies show however severe methodologic shortcomings.261 Some suggest that it is appendicitis and not appendectomy, which is protective.262 The mechanism of this association is unclear. Immunologic mechanisms have been proposed as the basis of the relationship between UC and appendectomy.
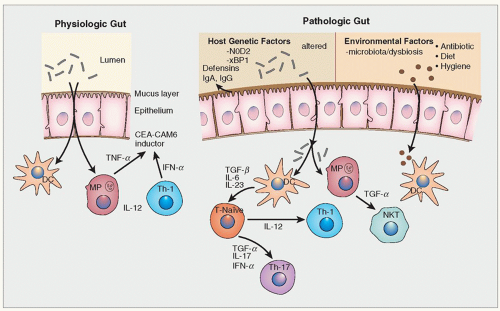 Figure 18-7. Complex interplay between microbes and various components of the innate and adaptive immune system in the pathogenesis of IBD. Normally secreted IgA, antimicrobial peptides secreted by Paneth cells, and mucin (MUC2) secreted by goblet cells provide protection against microbes trying to reach the epithelium. The epithelium with its tight junctions provides an additional protective barrier. When luminal bacteria do come in contact with the epithelium or enter the tissues release of various cytokines by the epithelium, and activation of tissue macrophages and dendritic cells lead to activation of the adaptive immune response. Macrophages are in addition able to kill the organisms by phagocytosis. Under physiologic condition the innate and adaptive responses are able to clear the bacteria without setting of chronic inflammation and secondary inflammatory injury to tissues. Under pathologic situation, either luminal bacteria or other environmental toxins/antigens are able to cross the mucin and epithelial barrier (leaky epithelium), activate dendritic cells, and macrophages. The dendritic cells lead to activation of naïve CD4+ T helper cells (TH) in the Peyer’s patches and mesenteric lymph nodes. TGF-β and IL-10 modulate the differentiation of CD4+ cells T-cell subgroups (H1, TH2, TH17, and regulatory T-cells) with their characteristic cytokine profile as shown. These activated T-cells then move back to the lamina propria to carry out their effector functions. MP, macrophage; NK, natural killer cell; DC, dendritic cell; IL, interleukin; TNF, tissue necrosis factor; TGF, transforming growth factor; Th, T-helper. |
Surgeon General of the Union Army while describing the history of medicine during American civil war described UC and illustrated the histology using photomicrographs, a remarkable achievement for the time.267 Within several years, the disease was well characterized and in 1909 at a symposium of Royal Society of Medicine, no less than 300 case have been collected from various London hospitals.266 The term UC is a poor one as ulceration is not a sine qua non for the disease and the word colitis fails to recognize that rectal involvement rather than colonic disease is the prerequisite for the diagnosis. However, the term has stuck and has been well ingrained into the medical literature such that until some major etiopathologic breakthrough leads to a newer nomenclature, there is no good reason to abandon it!
(pANCA) are positive in 70% of patients and this can distinguish patients from those having infectious colitis; however, it is less helpful in distinguishing from Crohn’s colitis since up to 50% of these patients may be pANCA positive.274 Endoscopy with biopsy though is the key diagnostic testing to be undertaken.
severe disease. Rarely, strictures occur on the basis of hyperplasia of the muscularis mucosae with submucosal fibrosis (Fig. 18-13).276 If true fibrous strictures are present in a colon showing diffuse inflammation, the diagnosis of CD, rather than UC, should be considered. Alternatively, stricture formation can be the result of coexistent diverticular disease or of malignant change.
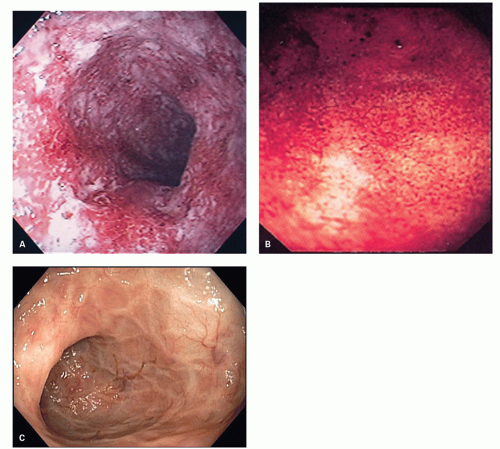 Figure 18-8. A: Endoscopic images showing active UC characterized by friable mucosa (bleeding on contact with the scope) and extensive purulent exudates. B: Prominent granularity and edema of the mucosa covered by mucoid material is seen here. C: Another example showing more chronic changes with loss of vascular pattern and mucosal folds, but no active lesions. |
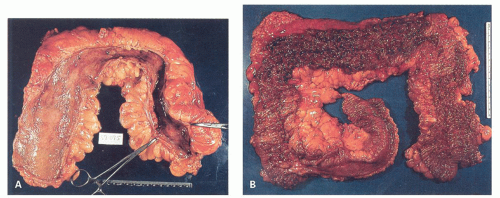 Figure 18-9. Ulcerative colitis. Gross appearances. A: Shortened, haustraless bowel with narrowing in the left colon. An inflammatory polyp is present in the transverse colon. B: Total UC extending throughout the large bowel, with extension in continuity for a considerable length of the terminal ileum. |
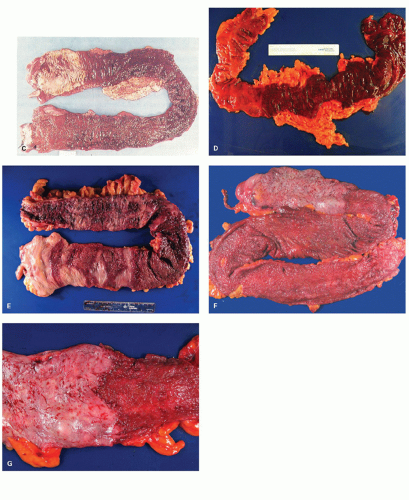 Figure 18-9. (Continued) C: UC affecting the large bowel in continuity from the rectum (bottom left) to the ascending colon (top left). Although the junction between the affected and unaffected bowel appears sharp, careful inspection of the remaining ascending colon reveals numerous well-defined areas of ulceration similar to a cecal patch. This could pose a diagnostic problem in multiple biopsy specimens, which would demonstrate markedly focal disease in this area, perhaps raising the question of CD. Fortunately, total colonoscopy is not usually carried out in patients with severe disease, but focality at either end in severe disease does occur. D: Another example of left-sided colitis with hemorrhagic friable mucosa that bleeds on touch. E: UC in a patient involving almost the entire colon with fulminant disease. The involvement of the right side shows many areas, which create an impression of patchiness; however, these merely represent areas of more severe inflammation. Histologically, the entire bowel showed mucosal inflammation typical of UC. F: Colitis involving almost the entire colon, sparing only the right side with the involved mucosa looking edematous red and granular. G: The close-up showing sharp demarcation between the involved and uninvolved segments. |
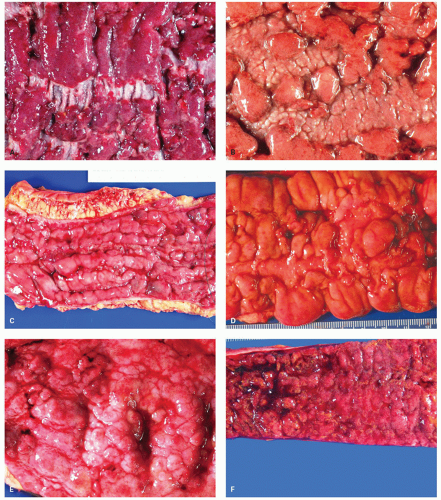 Figure 18-10. Closer look of mucosa in UC showing various types of ulceration and mucosal abnormalities. A: Extensive ulcerations represented by red friable mucosa with intervening pale areas of residual but inflamed mucosa. B: Broad and irregular ulcers with raised intervening areas of involved mucosa. C: Extensive linear tram track-like ulcers with intervening edematous mucosa. D: Irregular and geographic ulcers separating markedly boggy and inflamed mucosa. E: Mucosa with lumpy bumpy inflamed mucosa without deep ulcers. F: Extremely red and friable inflamed mucosa that has completely lost normal mucosal folds that is likely to bleed on touch. |
 Figure 18-11. Regrowth of the epithelium over undermining ulcers can create mucosal bridges such as seen here. |
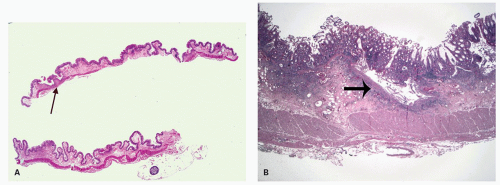 Figure 18-12. A: UC is characterized by the presence of mucosal ulcerations which extend into the submucosa (arrows). They may show a “collar-button appearance” with undermined edges. B: Another example at higher magnification. |
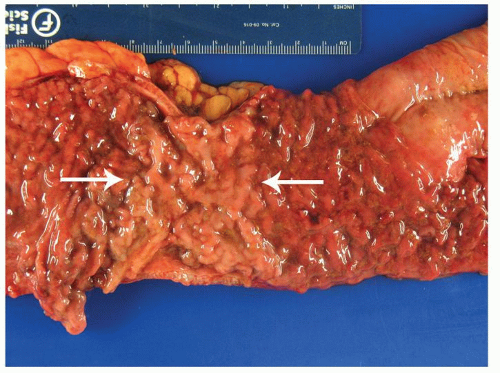 Figure 18-13. Benign strictures are rare in UC but can occur as shown here (arrows). The submucosal fibrosis leads to rigidity and luminal narrowing. There is no malignancy or involvement of the muscularis propria. |
terminal ileum to rectum from the major anatomical sites, (terminal ileum, ascending, transverse, descending, sigmoid colon, and rectum) in separate containers labeled as to site. UC involves the rectum and extends for a variable distance proximally, and this applies both to the architectural distortion and inflammatory infiltrate. Conversely, CD frequently has a focal distribution and often spares the rectum (see subsequent section).
inflammatory polyps. In severe disease, they burst into the loose submucosal tissues; there is a tendency to spread longitudinally beneath the mucosa, which sloughs off leaving an ulcer (Fig. 18-16). The mucosal margins of these ulcerated areas are further undermined and are relatively raised up to form polypoid tags of mucosa projecting into the lumen. These mucosal tags or inflammatory polyps can be short or extremely long and filiform.278
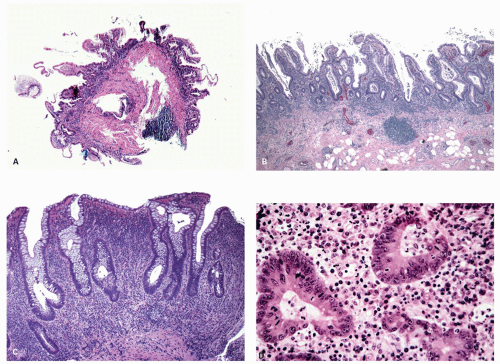 Figure 18-14. Ulcerative colitis. Low-power views (A,B) showing extensive shortening of crypts and loss of crypts. The surface can take a villiform appearance. In both pictures, mucosal inflammation is diffuse, transmucosal with basal accumulation of inflammatory cells (beneath the crypt base and the muscularis mucosae). Extension of the inflammation into the superficial submucosa as seen in this example (B) is not an evidence against UC. C: Classic biopsy findings in UC showing crypt branching and distorted crypts. The lamina propria shows dense inflammatory infiltrate composed of lymphocytes and plasma cells. Scattered eosinophils are visible even at this magnification. Note that crypts fail to reach the muscularis mucosae creating a subcryptal space occupied by dense plasma cell infiltrate. This basal plasmacytosis can be either focal or diffuse, and is a very useful diagnostic feature. It can however disappear following medical treatment. D: Neutrophils can infiltrate in between crypt epithelial cells (cryptitis) and accumulate in the crypt lumen (crypt abscess) which can lead to crypt destruction. |
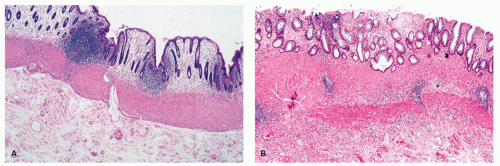 Figure 18-15. Ulcerative colitis. A,B: diffuse thickening of the muscularis mucosae can be very prominent with long-standing disease. It can be associated with an almost normal mucosa (A) or with persisting abnormality of the mucosal architecture in quiescent disease (B). |
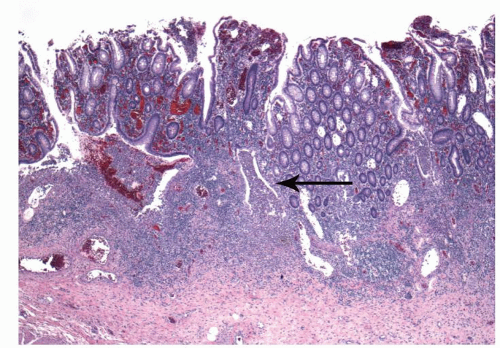 Figure 18-16. Crypt abscesses rupture into the submucosa (arrow) spreading laterally and eventually lead to ulceration as seen on the left side of the figure. |
plasma cells in UC demonstrate an increase in the major forms of IgA, IgG, and IgM.286 The increase correlates with disease activity and the rise of IgG- and IgM-containing cells is proportionally more than for IgA-containing cells.287
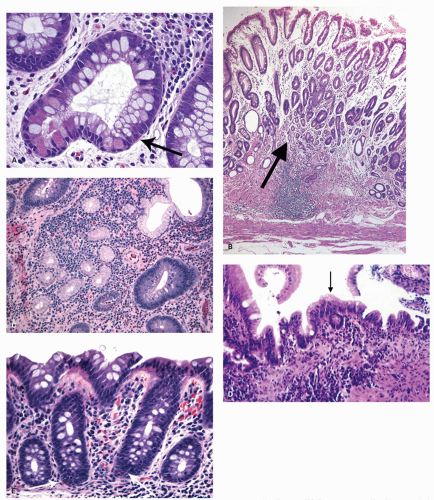 Figure 18-17. Metaplasia in IBD. A: Paneth cell metaplasia is the most frequent and can range from an occasional cell to many in each crypt. Endocrine cells may also be increased in the crypts and need to be differentiated from Paneth cells. The endocrine cells have the cytoplasmic granules toward the basement membrane and nucleus toward the lumen (arrow), while in Paneth cells the nucleus rests on the basement membrane and the granules are toward the crypt lumen. B,C: The appearance of the ulcer-associated cell lineage (UACL) or pyloric metaplasia is rare in the large bowel in UC and CD and more common in the ileum in CD. It can appear in the deeper part of the mucosa (arrow; B = low power; C = high power) but also on the surface (D), where the cells take the form of mucin secreting cells with a small amount of apical mucin (arrow). The phenomenon indicates the occurrence of an ulcer previously and is not specific for IBD. E: Increased number of endocrine cells in the crypts (arrows). |
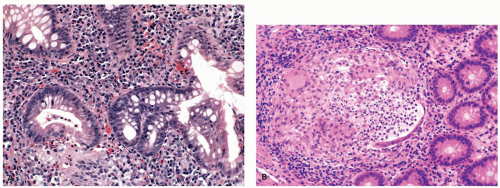 Figure 18-18. Crypt rupture may result in mucin granulomas that often have many neutrophils, few eosinophils, and loose aggregates of histiocytes and should not be confused with granulomas of CD (A). Occasionally, these can be more compact and have more histiocytes and even giant cells (B). |
the standard of practice and care. However, the paradigm shift toward getting a patient into a remission that is clinical, endoscopic, and histologic (no acute inflammation and a normal chronic inflammatory infiltrate in the lamina propria) is increasingly being considered as ideal.293
colitis.” Features like architectural distortion and Paneth cell/pyloric metaplasia have poor correlation with clinical disease, and their only value in reporting is to establish the presence of the underlying disease. The absence of any chronic changes or presence of minimal changes could imply complete histologic remission or even raise a doubt regarding the diagnosis of IBD. Sometimes during a follow-up biopsy, the clinicians may want to know if in fact ulcerative colitis is truly the correct underlying diagnosis, so “features of active colitis are absent, but crypt architecture changes as seen in inactive/quiescent ulcerative colitis” can be helpful. Alternatively, a sign out of “there are no features of active colitis or chronic changes” or that that the “biopsy is normal” can also be helpful. However, it must always be remembered that architecture can return completely to normal, so the absence of architectural changes never excludes the diagnosis of ulcerative colitis. Thus, “there is no evidence of IBD in these biopsies” works better than “normal biopsies” for that reason. One should recognize that the importance of routine, repeated biopsy examination in IBD is not just to assess disease activity, but sometimes to confirm the diagnosis or to raise the question of other forms of IBD, to exclude concurrent infection (especially those in which organisms may be visible), and to assess for the presence of dysplasia or carcinoma. Simple grading system for ulcerative colitis: This is based on the assumption that there is virtually never any acute inflammation (at least caused by IBD) without chronic inflammation also being present, so the paradigm of “no chronic inflammation—no acute inflammation” holds in IBD. No acute inflammation obviously implies that there is no cryptitis, crypt abscesses, erosions, or ulcers. Then logically if there is acute inflammation, it can be graded subjectively, but that in the presence of acute inflammation, grading chronic inflammation is unnecessary as it is always present to some degree, and is of no clinical significance as the presence of any acute inflammation implies an increased risk of relapse.
Table 18-6 Scoring System for the Assessment of Severity in Ulcerative Colitis | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Table 18-7A Simplified Grading System for Chronicity and Activity in IBD (Option A)* | ||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||
Table 18-7B Simplified Grading System for Ulcerative Colitis (Option B) | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||
A system for both grading biopsies and predicting relapse based on both the Geboes and Bessissow criteria is shown in Table 18-7B. However, one needs to be careful while dealing with biopsies from the right colon (cecum, ascending colon) that can have basal plasma cells normally, especially in adults. Biopsies from this region should therefore always be considered normal if based on chronic inflammation alone. As this tends to be an age-associated change, basal plasma cells may be more important in children in this location.
Various examples of biopsies with UC Biopsies from the cecum and ascending colon—colonic mucosa without abnormality Biopsies of large bowel from transverse colon—architectural distortion as seen in quiescent ulcerative colitis Biopsies of the descending colon—ulcerative colitis with an excess of chronic inflammatory cells but without basal plasmacytosis Biopsies from the sigmoid colon—chronic ulcerative colitis with moderate basal plasmacytosis* Biopsies from the rectum with mildly active ulcerative colitis* |
* In patients in clinical remission, the presence of these features has been reported to increase the likelihood of clinical relapse. |
Bessissow T, et al. Prognostic value of serologic and histologic markers on clinical relapse in ulcerative colitis patients with mucosal healing. Am J Gastroenterol. 2012;107(11):1684-1692. |
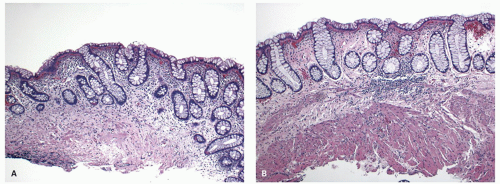 Figure 18-19. During quiescent phase, the lamina propria inflammation subsides and the only evidence, of prior colitis may be mild crypt distortion or Paneth cell metaplasia (A). In some instances the mucosa returns to normal architecture and only evidence of prior disease may be thickened or duplicated muscularis mucosae (B). |
be the only evidence of past inflammation or ulceration (Fig. 18-19B).297
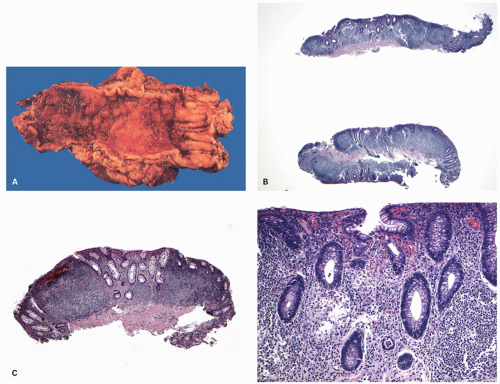 Figure 18-20. Follicular proctitis. A: Resected specimen of the rectum with a reddened granular mucosa that is otherwise indistinguishable from that of other resections for UC. B,C: Biopsies from another example that show marked lymphoid hyperplasia with germinal centres in some of them. The mucosa in between also shows a dense lymphoplasmacytic infiltrate; the crypts appear somewhat reduced in numbers with mild distortion of architecture. D: Higher magnification shows intervening areas with cryptitis and crypt abscess formation. |
and sometimes reepithelialized granulation tissue. These inflammatory polyps or mucosal tags may be present in large numbers and adopt bizarre shapes (Fig. 18-21A-D). The pathogenesis involves previous severe ulceration: islands of preserved inflamed and edematous mucosa that eventually take the shape of polyps and over time reepithelialization of the intervening ulcers (Fig. 18-22A-D).278, 301 The term “pseudopolyp” has been used to describe these postinflammatory polyps, but this appears to be a poor term. First, there is certainly nothing “pseudo” about these polyps, while “inflammatory polyp” is a better expression as it indicates the way in which the polyps are formed, and it satisfies the definition of polyp handsomely. However, they have to be distinguished from residual mucosal islands—which may be genuine “pseudopolyps.” These are the result of localized ulceration of the mucosa and usually submucosa, with undermining of adjacent intact mucosa. The surviving mucosa appears raised, but only relative to the adjacent ulcerated mucosa, so that it appears to form a polyp, which is really a mucosal island, and therefore appears to project into the lumen. The term mucosal island is better than pseudopolyp, removing the ambiguity inherent in that term.
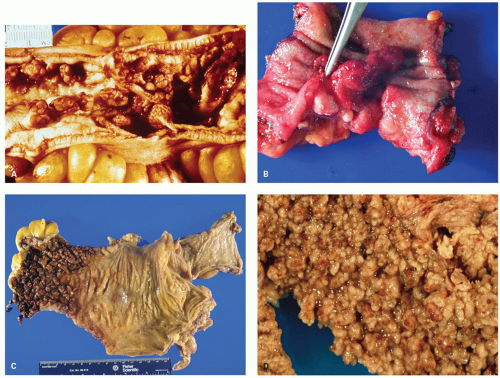 Figure 18-21. Inflammatory polyps in ulcerative colitis. A: Numerous varying sized polyps many of which are pedunculated and the gross appearance can closely mimic adenomatous polyposis syndrome. B: Another example with a large pedunculated solitary polyp. C: Carpet of numerous small polyps that sharply separate the involved segment from the normal mucosa in this example. D: Colitis with myriad inflammatory polyps. Note the impossibility of detecting neoplasms within such forests. |
much commoner in UC.301 They can also be found guarding the entrances and exits (and within) fistula tracts, so are sometimes called sentinel polyps. While confusion can occur grossly with adenomatous polyposis syndromes on gross examination, the appropriate histologic diagnosis should be sought by examining the background mucosa.
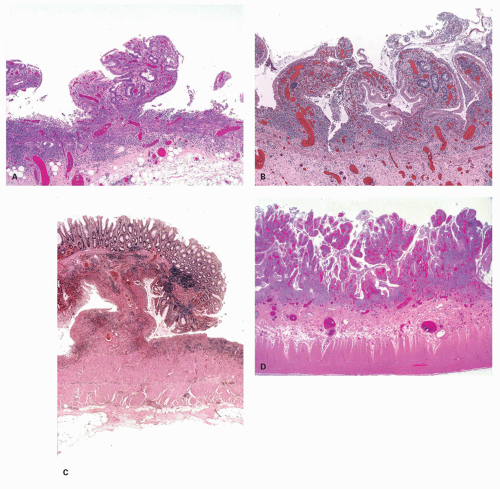 Figure 18-22. A: Early stages of inflammatory polyp formation showing extensive ulceration resulting in islands of residual inflamed and edematous mucosa that take the shape of a polyp. B: With time, the epithelium grows over ulcerated surface between multiple islands of polypoid mucosa. C: Some of the polyps can grow large with a mushroom shape, and can mimic adenomatous polyps grossly or on low power. D: Once the epithelium has completely grown over the ulcers and numerous such polyps are formed, the entire mucosa is covered with such polyps taking a lumpy bumpy shape (colitis polyposa). |
unless these are a form of hamartomatous polyposis, they must have been preceded by severe ulcerative inflammation, even if its etiology is obscure.
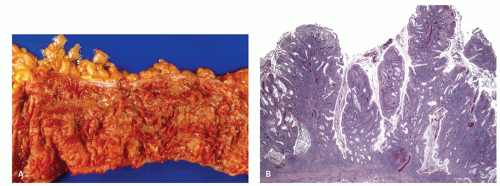 Figure 18-23. Inflammatory polyps in ulcerative colitis. A: Rarely, the polyps can have a finger-like or worm-like shape and referred to as filiform polyps. B: Microscopy show virtually entire mucosa is converted into filiform polypoid mucosa. |
skip lesions in the ascending colon have also been described in a small subset (4%). One study found that periappendiceal disease had a male predominance, and none had a prior appendectomy.313 The other situation of segmental or patchy inflammation is presentation as diverticular-associated colitis, described subsequently.
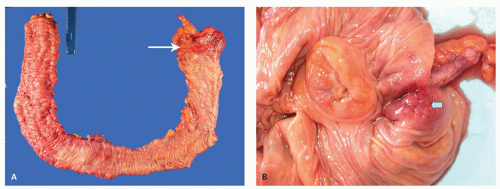 Figure 18-24. A: Subtotal colectomy in a patient with UC showing a distal colitis and inflammation in the cecum (cecal patch) (arrow) with mucosal erythema and thickened folds which extend to the appendiceal orifice as well. B: Mucosal inflammation around appendiceal orifice in a patient with left sided ulcerative colitis. |
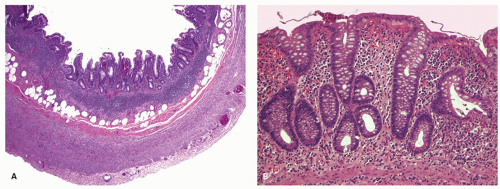 Figure 18-25. A: Involvement of the appendix with UC at low magnification showing the inflammation is largely mucosal with crypt architectural distortion. B: Higher magnification showing mucosal changes that are identical to those seen elsewhere in the colon. |
rectal mucosa, associated with PSC, while one study showed a distinct right-sided tendency of the persistent inflammation,298 the other failed to show any difference from controls.317 There is no way of knowing whether the rectum was ever involved in these patients or this represented spontaneous resolution of inflammation.318 Relative rectal sparing has also been documented in children more frequently (see later).
ileitis, but there are no good data on which to make that assessment. However we have seen ileal biopsies from patients with ulcerative colitis with occasional foci of acute inflammation in the lamina propria, but are unsure of its significance.
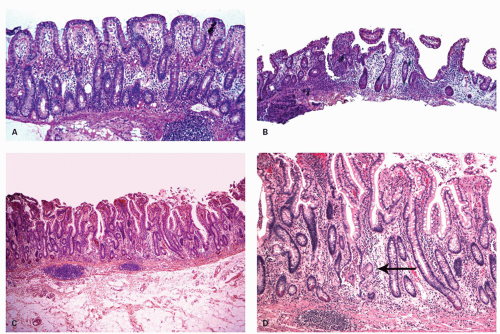 Figure 18-26. A: Ileal lesions associated with UC (so-called backwash ileitis) often show architectural distortion, regular shortening of the villi, cuboidal surface epithelial cells, and increased lamina propria inflammation. B: Another example of backwash ileitis with occasional branching crypt. The inflammation is mild. C,D: Backwash ileitis showing crypt and villous architectural distortion and areas of cryptitis. The inflammation is limited to the mucosa. A small focus of pseudopyloric metaplasia can also be seen (arrow). In this case the terminal 4 cm of the ileum was involved. |
counterpart ulcerative proctocolitis, the changes are usually readily discernable on biopsy. The “nonspecific” part of this designation is therefore an historical title borne out of ignorance when all biopsies were called “nonspecific chronic active colitis/proctitis” (regrettably still all too common). There was no appreciation that the chronic infections of this region whether venereal, tuberculous, or even amebic could be diagnosed and treated. Now we recognize that a vast majority of chronic proctitis encountered in clinical practice in Westernized societies represents IBD (UC/proctitis) and crypt architectural distortion, deep lamina propria plasma cells, cryptitis, and crypt abscesses are characteristic histologic changes. The other main form of IBD, CD, rarely presents as proctitis alone. However, it should also be recognized that the changes are not entirely specific, and as listed in the table other causes need to be considered in the differential diagnosis. Some of the chronic infections at times very closely mimic IBD and require a detailed clinicopathologic workup including demonstration of the pathogen in the tissues. Rarely, the changes of ulcerative proctitis can be those of a follicular proctitis.
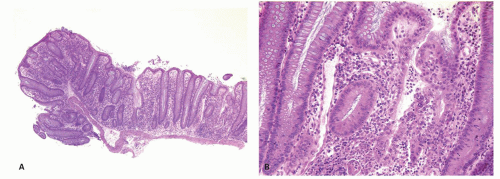 Figure 18-27. Ulcerative colitis in children. A: Diagnostic microscopic features such as diffuse mucosal inflammation and widespread architectural abnormalities may be absent from biopsy samples obtained in young children. The picture is from a first set of biopsies obtained in a 2-year-old boy with bloody diarrhea, which subsequently turned out to be UC. The photograph shows focal basal accumulation of inflammatory cells. High power illustrates disease activity (B). |
Table 18-8 Causes of Proctitis | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
frequency and urgency with blood but little or no diarrhea. In addition, chronic ulcerative proctitis may sometimes be remarkably resistant to medical therapy, including 5-aminosalicylic acid, local and even systemic steroids, or immunosuppressive agents. Some patients with only rectal involvement benefit greatly from restorative proctocolectomy.328 Morphologically, it has the features of UC, although the chronic inflammatory component may be more severe than those with more extensive disease even in remission.277
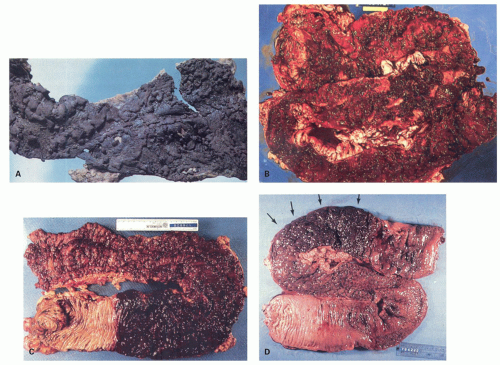 Figure 18-28. Fulminant UC (A-F) and CD (G,H). A: Toxic dilatation, in UC, in which the bowel wall tears even on the most gentle handling (top right), and perforation (lower left of center). B: Fulminant total UC in the absence of dilatation, with deep ulceration going into and through the muscularis propria. C: Toxic dilatation with maximal disease in the vicinity of the hepatic flexure and a sharp margin of demarcation proximally in the ascending colon. D: Toxic dilatation with maximal disease in the descending and sigmoid colon (arrows), but with a very indistinct proximal margin in the ascending colon. |
not invariably involved.332 There may be proximal or distal sparing, or both, even in cases of UC and can be misleading.316, 333 Further, the transition may be in the form of aphthoid ulcers. The inflammation can be focal or diffuse, the mucosa can be either diffusely hemorrhagic or there may be linear ulcers. The intestine may have the consistency of wet paper, tearing readily with subsequent peritonitis. Extensive loss of mucosa can occur and any surviving mucosa shows intense vascular congestion and edema, although sometimes with a relatively mild inflammatory cell response. In areas of mucosal ulceration, the submucosal tissues largely disappear laying bare the deep muscle coats, which may be covered by only a thin layer of very vascular granulation tissue, and may also be visible grossly.
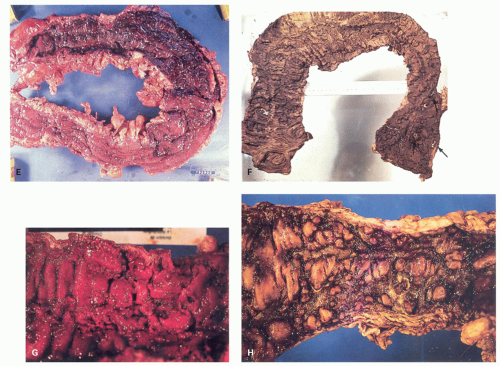 Figure 18-28. (Continued) E: Fulminant colitis which had perforated proximally, but with train-track ulcers distally. In fulminant disease, this does not necessarily indicate CD. F: Fixed specimen showing residual mucosal islands, with ulceration that tends to be longitudinal. Multiple perforations are present, and light is visible through them (arrows). G,H: Fulminant colitis in CD. In both illustrations, there is a suggestion of residual mucosal islands reminiscent of cobblestoning, but other features were also present to support that diagnosis. |
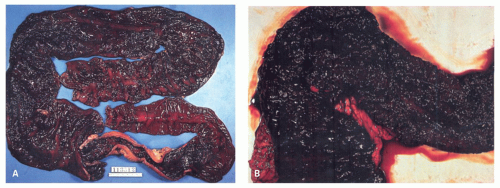 Figure 18-29. IBD presenting with severe hemorrhage (A,B) in UC. Note the diffusely hemorrhagic mucosa extending well back into the terminal ileum. |
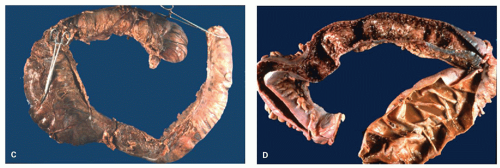 Figure 18-29. (Continued) C: Colectomy specimen in a case of fulminant UC with toxic megacolon. The dilatation as demonstrated by filling the colon with formalin is maximal in the transverse colon. D: The same specimen is opened up to reveal markedly inflamed and ulcerated mucosa with areas of the bowel wall that are paper thin. |
Table 18-9 Clinical Criteria for the Diagnosis of Fulminant Colitis | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||
colitis, some have overt diffuse architectural changes indicative of prior UC (Fig. 18-30B). These can be signed out as severe active UC. Where it is focal, the possibility of CD needs to be considered, but still requires the features described above.
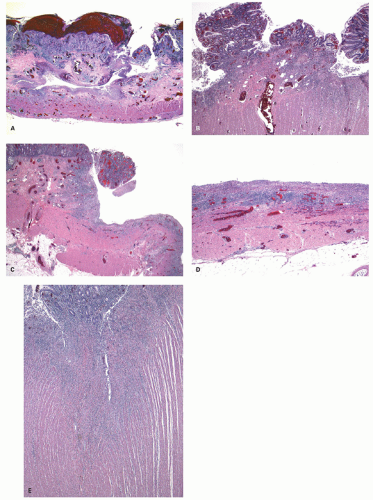 Figure 18-30. Histology of fulminant colitis. A: Deep undermining ulceration that is frequently hemorrhagic. The ulcer is seen reaching almost upto the muscularis propria in this area. Few lymphoid aggregates can be seen in the area of the ulceration. B: There is marked architectural distortion in the pseudopolyp present, implying chronic inflammation and possibly resolved ulceration. The distribution of these changes is useful as in this example the underlying disease is very likely to be UC. Also note that the inflammation in the area of ulceration extends into the muscularis propria (transmural); however, this is different from the typical lymphoid aggregates of CD. C,D: Extensive ulceration as seen here can be a feature in some cases with only scant islands of residual mucosa. The ulcer is seen resting upon the muscularis propria. E: Fissuring ulcers. These can be seen in fulminant IBD of any etiology, and can go into or through the muscularis propria and occasionally even perforate in the absence of toxic dilatation. |
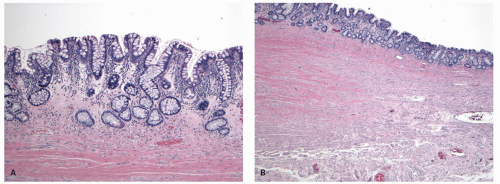 Figure 18-31. Histologic changes post TNF-α therapy showing marked reduction in inflammation and empty looking lamina propria (A), although grossly ulcer were present and patient was still very symptomatic (B). Also note the marked submucosal fibrosis. |
syndrome, the accuracy of the evaluation, and the duration of follow-up. Reported incidence rates vary between <10% in patients undergoing pouches for familial polyposis and up to around 60% in patients who had severe colitis with backwash ileitis. The risk for development of pouchitis is highest during the first 2 years postoperatively. Three to twenty percent of patients with pouchitis develop persistent or recurrent episodes of pouchitis that frequently require immunosuppressive treatment. It may or may not be accompanied by clinical symptoms. Clinically, pouchitis typically results in increased stool frequency, liquidity, urgency, abdominal and/or pelvic discomfort, and often fecal incontinence. Therapy is with antibiotics, usually ciprofloxacin and metronidazole. Other adverse sequelae include mechanical, inflammatory, functional, neoplastic, and metabolic conditions. Common causes of failure include pouchitis, pelvic sepsis, and poor function. Occasionally, patients with chronic pouchitis develop Crohn’s-like GI and systemic complications including enteric stenoses or fistulas in the small bowel immediately proximal to the pouch, perianal fistulas, pouch stenoses or fistulas, arthritis, and pyoderma gangrenosum. Various subtypes of pouchitis have therefore been distinguished. The most common form has been called “usual pouchitis.” Persistent or recurrent disease is termed “chronic or refractory pouchitis.”345
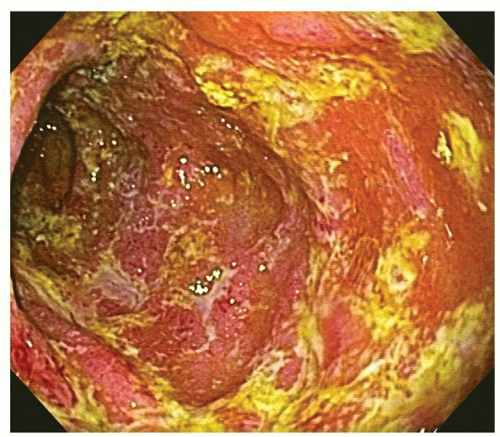 Figure 18-32. Endoscopic appearance of pouchitis showing marked mucosal inflammation and exudates. |
unlike usual small bowel, does not produce the sulfated mucins. It is also supported by experimental data showing a different pattern of the expression of human tropomyosin isoform 5 (hTM5) in the ileal pouch. In genuine ileal samples, hTM5 is not expressed or focally expressed only in goblet cells. Pouch biopsies obtained at 6 months after surgery in one study showed a diffuse hTM5 staining in the goblet cells and in the nongoblet cells lining the crypts and the lumen. These changes are associated with shortening and reduced number of the villi.351 It has been suggested that these changes represent an adaptive response. “Colonic metaplasia” occurs more frequently in cases with severe pouchitis, suggesting that it may be a “reparative” rather than an “adaptive” response, although this can be interpreted either way.352
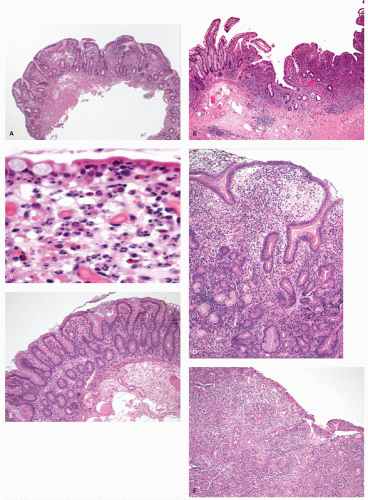 Figure 18-33. A: Pouch biopsies often show small intestinal mucosa with mild architectural distortion with shortening of the villi and infiltration of the lamina propria by a variety of cells such as lymphocytes, plasma cells, eosinophils and histiocytes. B: Active pouchitis can show intense mixed inflammation of the mucosa, which can be patchy, associated with neutrophils in the lamina propria (C), and subsequently into the crypts. D: With time more prominent architectural abnormalities and occasionally pseudopyloric metaplasia can be seen. E: The pouch mucosa sometimes may start looking more like colonic mucosa (colon metaplasia). F: In severe cases, extensive mucosal ulceration can be seen. |
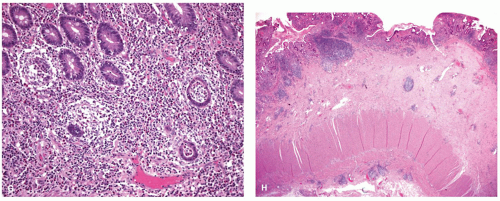 Figure 18-33. (Continued) G: Crypt rupture granulomas can be seen like many other inflammatory conditions, and should not lead to the diagnosis of CD. H: Sections from a resected pouch shows transmural lymphoid aggregates which can further mimic CD. |
discussion). The presence of “cuffitis” (inflammation in the residual couple of cms of rectal cuff—most distal rectum) can cause symptoms similar to ulcerative proctitis, but can be surprisingly difficult to treat. An occasional problem is that of the presence of “prepouch ileitis” (see subsequent discussion).
invasion may be present. However, occasionally carcinomas just appear “out of the blue” and rarely with metastasis. Because dysplasia is so uncommon in pouches there are no good guidelines, so each patient has to be managed by weighing the pros and cons of all options for therapy, including local excision if a lesion is visible.
overtly inflamed. Occasionally, there may be some form of obstruction or stricture at the inlet, but usually this is quite patent.
small intestinal involvement, rectal sparing, and skip lesions are other helpful features. The patchiness that may be evident in UC is more subtle than the discrete skip lesions of CD. Inflammation only evident in the rectosigmoid and the splenic flexure with a long segment of normal left colon is more of a skip lesion (and consistent with CD) than patchiness. It is thus appropriate to obtain multiple biopsies from different segments of the colon and the terminal ileum. Furthermore, in difficult situations, biopsies of the upper GI tract may be indicated to assess the extent of the disease and to solve diagnostic problems. These may help if the changes are typical; however, gastroduodenal changes can also be found in UC (see later).
examination, the transition between affected and unaffected areas in the colon is usually less clear-cut.
Table 18-10 Vienna and Montreal Classification for Crohn’s Disease | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
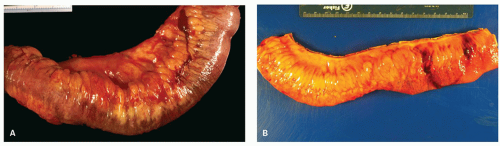 Figure 18-34. A,B: Mesenteric fat partially surrounds the intestine, extending from the mesenteric attachment anteriorly and posteriorly corresponding to the involved segment. Variable degree of encroachment of the circumference of the intestine occurs, and as seen as here focally it completely encircles the small bowel. This phenomenon, known as fat wrapping, is fairly specific for CD. |
within a single specimen from deep serpiginous fissuring ulcers to tiny aphthous ulcers surrounded by normal or mildly edematous bowel (Figs. 18-36 and 18-37). Larger ulcers are usually discrete with edematous, overhanging, slightly violaceous edges, and they are often stellate in outline.367, 368, 377, 378, 379 Other examples have a more linear “tramline” appearance with two, and often three, roughly parallel lines of discrete ulceration running along the length of the colon. These are usually related to the point of entry of mesocolic vessels into the bowel wall. When the linear parallel ulcers are joined by a horizontal ulcer at the top, they resemble “bear-claw” markings or so-called “bear-claw ulcers.” After ulcers heal, tramline indentations of the mucosal surface frequently remain. Another appearance that is typical but not characteristic of CD is cobblestoning of the mucosal surface (Figs. 18-36 and 18-37). This results from areas of marked edema of the mucosa and submucosa separated by crevices that represent narrow fissuring ulcers, or aphthous ulcers that coalesce either horizontally or vertically or both. Fistulae are found in up to 60% of patients, whereas overt perforation of active colonic CD is uncommon, and usually right sided. This probably reflects the fact that the inflammatory process penetrates the tissue planes slowly and causes loops of inflamed bowel to adhere to one another, effectively walling off any perforation or abscess that may have formed. Fistulae, perforations, and abscesses form the base of the fissuring ulcers, where there is extension of the inflammatory process into the serosa and adjacent structures (Fig. 18-38). It can be difficult to find fistulae. Gentle probing, especially if recesses in the mucosa are seen may be helpful. Sometimes, pushing aside inflammatory polyps and looking for openings that may be immediately adjacent to them (sentinel polyps) may be helpful. They may also be visualized when strictures are bread loafed as thinly as possible (about 2 mm thickness). Indeed, it is quite a good practice to do this routinely to find unexpected fistulas and even an occasional carcinoma. In the fixed specimen, serial sections a few millimeters apart going transversely across the bowel but without destroying the integrity of the specimen is a simple and quick way of finding intramural fissures and fistulas.
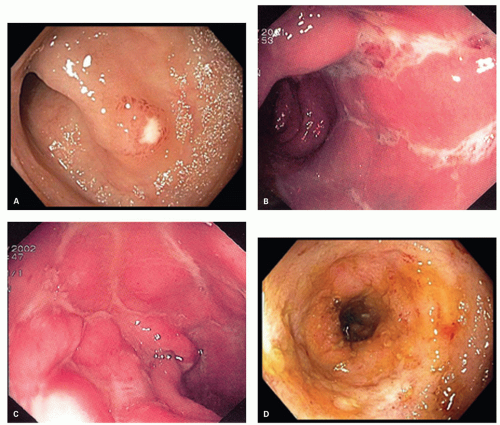 Figure 18-35. Crohn’s disease. Endoscopic pictures of a small aphthoid ulcer (A) and of large irregular, serpiginous ulcers (B,C). D: Chronic disease with abnormal granular mucosa loss of folds. |
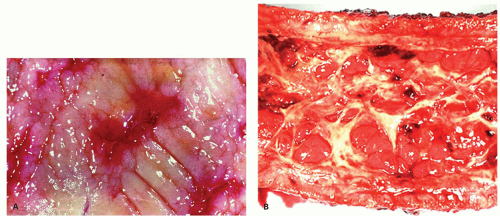 Figure 18-36. Crohn’s disease. Gross features include the presence of small irregular ulcers which may be the result of confluent aphthoid ulcers (A). They may become longitudinal ulcers (B). |
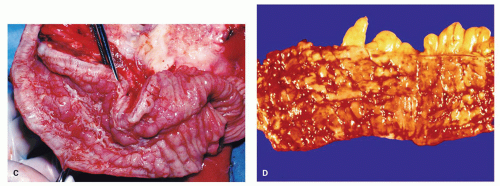 Figure 18-36. (Continued) The combination of longitudinal and transverse ulceration in an edematous mucosa is responsible for the characteristic cobblestone appearance (C,D). |
distinction from UC is problematic clinically (unless fistulas or granulomas are present) serology is not helpful.274
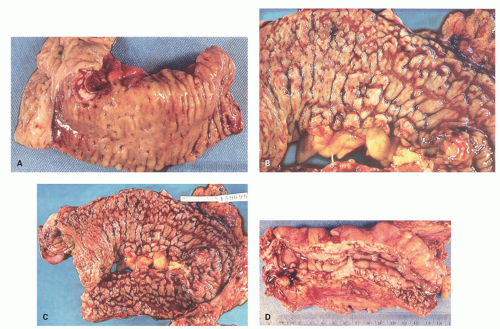 Figure 18-37. Crohn’s disease. Aphthoid ulcer-cobblestone phase of CD. A: In this ileocolic anastomosis resection because of a fistula at the anastomosis, recurrent aphthoid ulcers are visible, limited almost entirely to the terminal ileum, stopping abruptly at the colonic margin. They vary from pinpoint areas of redness to small, punched-out ulcers. B: If activity continues, the ulcers enlarge (left), become stellate, and link with each other both transversely and longitudinally, forming islands of mucosa which are the cobblestones. This appearance is accentuated by the marked submucosal edema present in the areas of cobblestoning. The longitudinal ulceration is usually more marked, forming tram track ulcers (right). C: Continuation of the same process results in deep transverse ulcers in addition, with reemergence of cobblestoning, although these areas are now discrete residual mucosal islands (bottom). D: If the process continues, there is marked stricturing resulting from a combination of cobblestoning, thickening of the wall with inflammation, fibrosis, and extensive creeping fat, all of which prevent expansion of the lumen. |
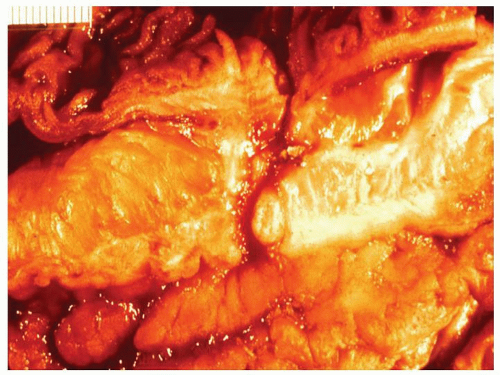 Figure 18-38. Fistula formation between loop of a small bowel and transverse colon. |
noticeable when multiple biopsies are examined from the same patient, either synchronously or metachronously.277, 381, 382, 383 However, usually the initial exercise is in deciding if the patient has features of IBD (architectural distortion and deep plasma cells, the latter distal to the region of the ileocecal valve, and then decide which type of IBD is present). In deep biopsies it may be seen to extend into the submucosa, where its density may be proportionately greater than in the mucosa. Sometimes the infiltrate contains eosinophils or mast cells, which can be numerous but are not distinctive. Granulomas are a bonus, and great care needs to be taken to ensure that they are not at the site of ruptured crypts, and therefore mucin granulomas. They are not a sine qua non of CD in a patient who clearly has IBD.
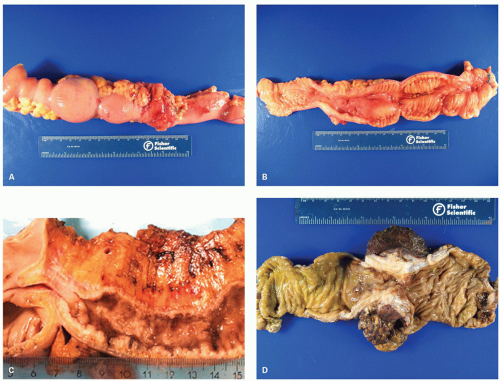 Figure 18-39. Stricture may develop in CD as shown here that may be multiple as seen from outside (A) and after opening the small bowel (B). (C) and (D) show strictures in terminal ileum and colon, respectively. |
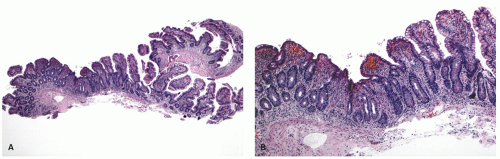 Figure 18-40. The key feature of CD on biopsies is patchiness or variability in inflammation, which is not always appreciated or present. A: Ileal biopsies showing parts of the biopsy with normal villous architecture and lack of mucosal inflammation. On closer look (B) one can easily see area with increased mucosal inflammation, loss of villi and crypt distortion. |
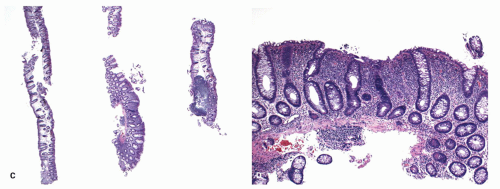 Figure 18-40. (Continued) C: Colonic biopsies in a patient with CD showing three fragments of which one shows diffuse mucosal inflammatory changes while the others are either normal or have focal inflammation. D: Higher magnification of the inflamed fragment to show increased lamina propria inflammatory infiltrate, subtle crypt distortion, and Paneth cell metaplasia. Note that in comparison to UC, the goblet cells are relatively well preserved (less mucin depletion) and crypt architectural distortion is milder. |
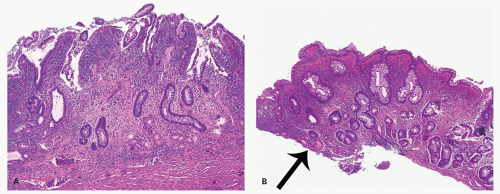 Figure 18-41. Another feature of CD that is strongly suggestive, but not diagnostic is pseudopyloric metaplasia in small-bowel biopsies which can be fairly easy to recognize (A) or be very focal and easy to miss as seen on edge of this biopsy fragment (arrow) (B). Both these examples also show extensive architectural abnormalities of the villi of the ileum, ulcerations, and intense lamina propria inflammation. |
thickened duplicated muscularis mucosae) support this diagnosis, the problem being that virtually everything in the list of etiologies that can also be recurrent is in the differential diagnosis.
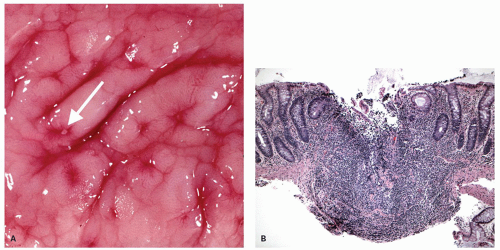 Figure 18-42. A: Gross aspect of aphthoid ulcers in CD. They appear as small, round mucosal depression with yellow or grey base surrounded by a reddish halo in an otherwise normal or edematous mucosa. B: Histology of aphthoid ulcers showing the classical site of the ulcer over a lymphoid nodule developing in the M-cell region of the large bowel. These were incidental histologic findings in a mucosa with occasional red, pinpoint-like areas. Note the lack of involvement of crypts immediately adjacent to the ulcer, which appear normal. |
a number of other conditions.393, 394 Migration of neutrophils into crypt lumina may result in crypt abscess formation, and rupture of inflamed crypts releases mucus into the surrounding lamina propria. As described above in the section on UC, this can sometimes result in pericryptal aggregates of macrophages (crypt rupture granulomas or mucin granulomas), and it is important to recognize these for what they are and not attribute to them the same diagnostic relevance as “proper” granulomas (Fig. 18-18A,B).284, 395, 396 While these may be more common in CD, they are also seen in genuine UC or active colitis from any other cause.20, 397 Its diagnostic value is therefore limited.
Table 18-11 Common Causes of Endoscopic Aphthoid Ulcers | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
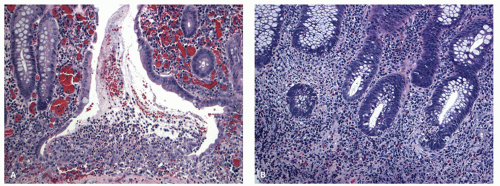 Figure 18-43. A: Early lesions in CD can appear as mucosal ulcers with a stream of leucocytes toward the lumen. They have been called “mountain peak ulcers.” Although this lesion is suggestive of a diagnosis of CD, it is not specific. B: Neutrophils infiltrating into the bases of multiple crypts (cryptitis) as well as lamina propria as seen here represent active disease. |
aspect, but a “loose” expanded form of granuloma is more common in CD. Granulomas can be detected in otherwise endoscopically normal-appearing mucosa or in inflamed tissues. Some cases of CD tend to show scattered mucosal granulomas without a background of mucosal inflammation and IBD-like changes, and this always raises a differential diagnosis of infections and sarcoidosis. Central necrosis and caseation are unusual and should raise the suspicion of tuberculosis. Giant cells may contain calcified conchoid bodies.384 Associated inflammatory cells are lymphocytes (usually CD4+ T cells and the epithelioid cells may express MHC class II antigens).403
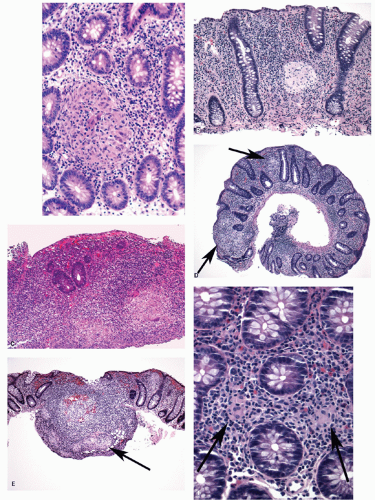 Figure 18-44. Another key feature of CD on biopsies is the presence of granulomas which can be solid and well formed, and easily recognized even on low power (A-C), or they can be subtle (arrows) (D,E). Sometimes, only loose aggregates of few epithelioid histiocytes (arrows) may be seen (microgranuloma) (F), which are not really pathognomonic for a diagnosis of CD. |
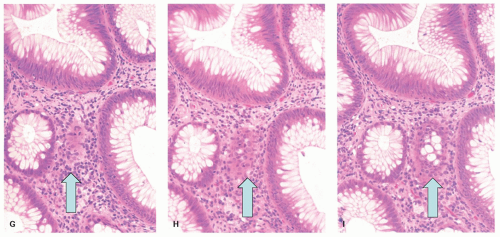 Figure 18-44. (Continued) G-I: Tangentially sectioned crypts can be confused with granulomas as shown here and only become evident on serial sectioning. |
and surrounded by inflammatory granulation tissue (Fig. 18-45A). Fissuring ulcers extend into and often through the colonic wall to form sinuses or fistulae, and may terminate in an extramural abscess, or communicate with other fissuring ulcers extending laterally to produce a complex network of sinuses and fistulae (Fig. 18-45B-D). In other cases, there may be more widespread mucosal ulceration with large, deep, but still discrete, mucosal defects with overhanging edematous edges. Despite the severity of the ulceration, it is often remarkable that in CD, the adjacent mucosa within a few millimeters may be virtually normal. Ulcer healing may lead to submucosal entrapment or misplacement of epithelium which may form mucusfilled cysts (colitis cystica profunda). The other mucosal inflammatory changes are the same as described in the previous section, except that the patchiness or skip lesions are better appreciated in resection.
Table 18-12 Granuloma-associated Diseases in the Gastrointestinal Tract | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
frequency of <1%. It usually involves the kidney, but amyloidosis can also be seen in the bowel wall rarely426 (Fig. 18-52).
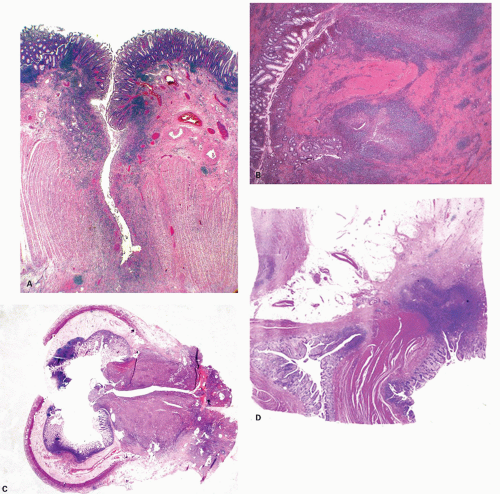 Figure 18-45. Deep fissuring ulcers (A,B) can become deeper to go through the entire thickness of the muscle layer and join each other to form a complex network of sinuses. Eventually they may perforate (C) and form fistulas between involved intestinal segments and adjacent organs or nearby uninvolved loops (D). |
lesions of arteries supplying areas of intestine affected by CD were demonstrated. Granulomas were identified in the wall and lumen of the blood vessels and the vascular lesions were present in all 15 patients examined. Granulomatous angiitis was later confirmed by the same authors in 24 consecutive surgical samples. Based on these observations, multifocal GI infarction was proposed as the pathogenetic mechanism for CD but this hypothesis has not been confirmed.291, 431 While the nature and the exact frequency of granulomatous
vasculitis remain to be determined, their occurrence and diagnostic significance are unquestionable. Occasionally, giant cell arteritis has also been observed in CD and rare cases of concomitant occurrence of Takayasu’s arteritis and CD have been reported.432
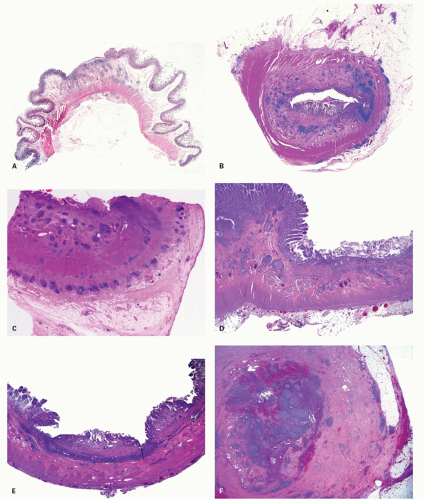 Figure 18-46. CD with transmural lymphoid infiltration. A,B: This is usually found only in areas of gross macroscopic disease as shown here with ulcerating small-bowel disease with focal ulceration. Particularly in the submucosa, there are numerous aggregates of lymphocytes without germinal centers, primarily expanding the submucosa, although smaller aggregates are present immediately beneath the muscularis propria in the subserosa, creating the full picture of transmural inflammation. Even at this magnification, this appearance is virtually diagnostic of CD. C: Small-bowel disease with lymphoid aggregates, but here forming three rosary beadlike rows: one in the submucosa, a middle row in the region of the myenteric plexus, and a third in the subserosa. D: As seen here, sometimes prominent lymphoid aggregates are present in the submucosa with relative sparing of the muscularis propria. The pattern of inflammation can be extremely variable. E: Uncommonly, the most extensive disease is limited to the submucosa. This is found particularly in resections of defunctioned bowel with CD. F: Appendiceal involvement by CD as shown here on low magnification showing transmural lymphoid aggregates. The mucosal changes tend to be similar to colonic disease. |
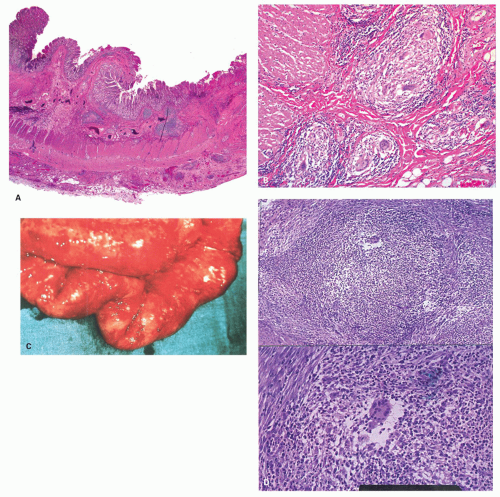 Figure 18-47. Granulomas in resection specimens are seen most commonly in the submucosa as shown in a resection of small bowel at low magnification (A) and higher magnification (B). They can also be seen in the muscularis propria (C), or rarely as small whitish subserosal nodules (miliary CD) (D). The histology of the subserosal nodules shows granulomas. |
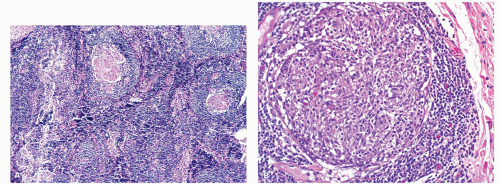 Figure 18-48. A: Granulomas can appear in mesenteric lymph nodes. B: Higher magnification. |
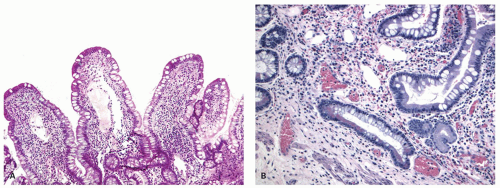 Figure 18-49. One of the more common histologic features is the occurrence of dilated lymphatics or lymphangiectasias in the mucosa (A,B) but also in the submucosa or rarely in subserosa. |
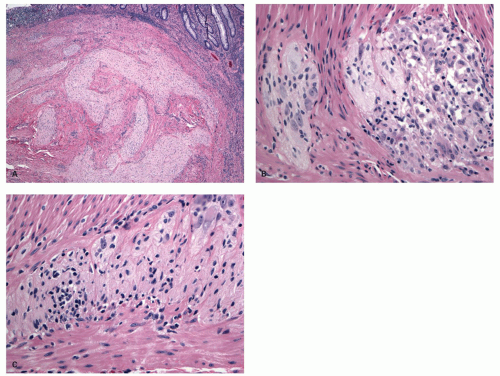 Figure 18-50. A: Abnormalities of the intrinsic enteric nervous system are common and characteristic. They include an increase in size of submucosal nerve fibers, sometimes called neuromatous hyperplasia and as seen here can resemble a traumatic neuroma. They are associated with granulomatous inflammation (B) or show infiltration by chronic inflammatory cells (C). |
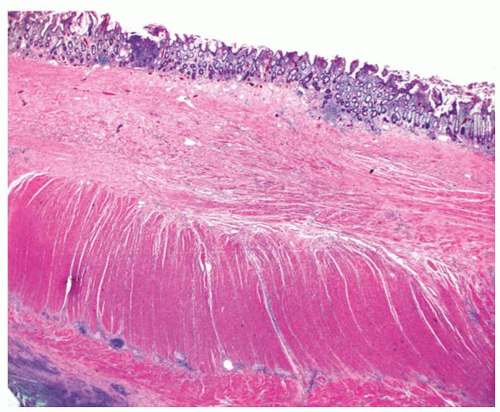 Figure 18-51. Ileal resection in a patient treated with a TNF-α antagonist. Note the dense fibromuscular changes occupying the entire submucosa, the virtual absence of the usual submucosa, myenteric plexus, and subserosal lymphoid hyperplasia, with only vestigial remnants and minimal inflammation in the lamina propria. |
Related posts:
 Disorders of Endocrine Cells
Disorders of Endocrine Cells
 Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
 Mesenchymal Tumors
Mesenchymal Tumors
 Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
 Enteric Infections and Associated Diseases
Enteric Infections and Associated Diseases
 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


