fungal infections such as candidiasis, certain viral diseases, and parasitic infections, whereas humoral immunity seems more important in protecting against run-of-the-mill enteric bacterial and viral infections.12
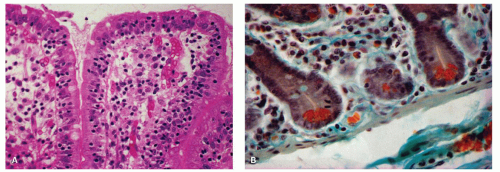 Figure 3-1. The diffuse lymphoid system of the intestinal tract. A: Intraepithelial lymphocytes (IELs). Mucosal biopsy specimen from a patient with tropical sprue, showing intestinal villi with an increased number of lymphocytes within the surface epithelium. B: Section of normal jejunal mucosa showing lymphocytes, plasma cells and eosinophils within the lamina propria between the intestinal crypts. Using this stain, Paneth cells in the crypt bases are bright orange red. (Masson’s trichrome stain) |
Although they appear to be few in number in any one section (at the range of 10-25 per 100 epithelial cells in the small bowel and ˜5 per 100 epithelial cells in the colon),22, 23, 24 when the entire intestine is considered, they are in fact very numerous and are said to equal in aggregate the number of lymphocytes found in the spleen. Histologically, the IELs consist of dense nuclei with minimal cytoplasm and do not have any epithelial attachment. The predominant phenotype is the cytotoxic T cell expressing αβ T-cell receptors, which are CD3+, CD8+, CD103+, CD4−, and CD5−. A smaller population (10%-15%) consists of T cells expressing γδ T-cell receptors that are negative for both CD4 and CD8. A third population of CD56+ IELs is also recognized that are virtually undetectable in normal mucosa. They have T-cytotoxic and natural killer (NK) properties.20, 25 The IELs overlying the lymphoid follicles consist predominantly of B cells. In addition, other intraepithelial cells such as macrophages, mast cells, neutrophils, and eosinophils may also be present.16, 23, 26 IELs are greatly increased in several diseases, such as celiac sprue, tropical sprue, lymphocytic colitis, and collagenous colitis. They are typically not increased in inflammatory bowel disease.23 In inflammatory states, neutrophils and eosinophils may also enter this compartment.27
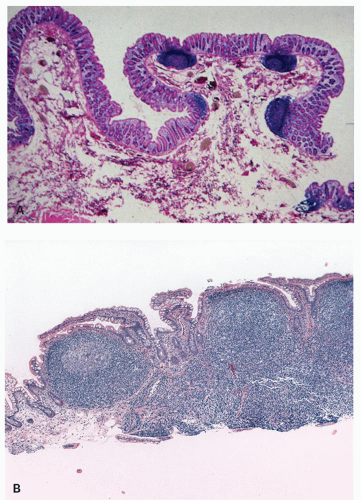 Figure 3-2. Solitary and aggregate lymphoid follicles of the human intestinal tract. A: Colonic mucosa and submucosa containing three solitary lymphoid follicles. The latter extend beneath the muscularis mucosae, and there is dimpling of the surface epithelium over the follicles. B: Peyer’s patch, composed of numerous lymphoid follicles aggregated together in a linear fashion. |
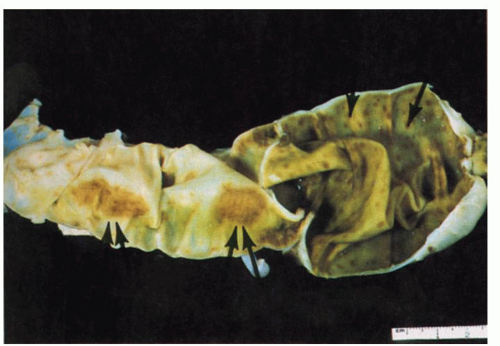 Figure 3-3. Autopsy specimen of terminal ileum and cecum. Two Peyer’s patches are visible in the ileum, measuring more than 3 cm in length (double arrows). Solitary lymphoid follicles are discernible in the cecum as tiny brown spots (arrow). |
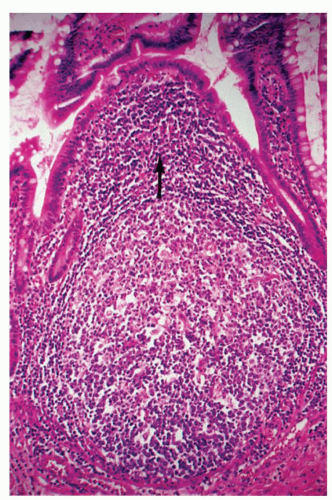 Figure 3-4. Intestinal lymphoid follicle. This is composed of a large follicular zone and the dome region, which is the area lying between the follicle and the surface epithelium (arrow). The mucosal surface overlying the follicle is dome shaped, devoid of villi and crypts, and lined by cuboidal epithelium. |
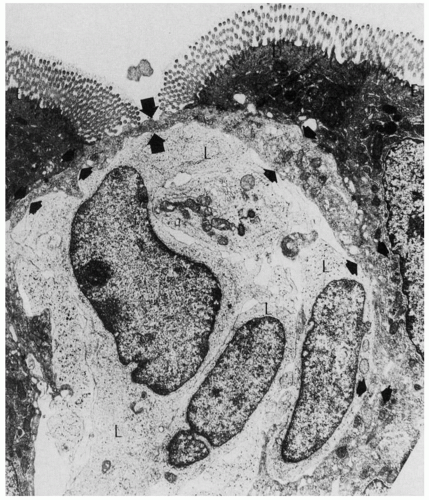 Figure 3-5. Electron micrograph of an M cell. This is a thin, membrane-like cell (arrows), the luminal surface of which is covered by microfolds and not microvilli. In the space below the M cell are three lymphocytes (L). (Courtesy R. L. Owen, M.D.) |
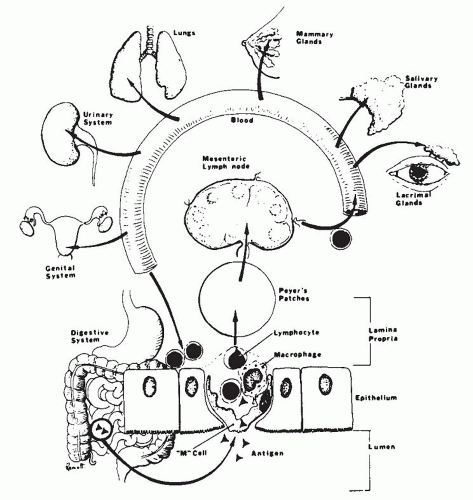 Figure 3-6. Mucosa-associated lymphoid system. |
use of immunohistochemistry. Sometimes, unexpected histologic changes may be found in the gut, such as nodular lymphoid hyperplasia and giardiasis, which should lead one to suspect an immunodeficiency disorder in a clinically unsuspected case. As common variable immunodeficiency (CVID) is so common, it may sometimes be detected in relatively asymptomatic patients because of a paucity of IgA plasma cells in the lamina propria with no compensatory increase in other classes of plasma cells.
into four major categories as described in the paragraphs that follow.
Table 3-1 Immunologic Tests for the Categorization of Primary Immunodeficiency Disease | |
|---|---|
|
Table 3-2 Pathology of the GI Tract in Primary Immunodeficiency Disorders | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
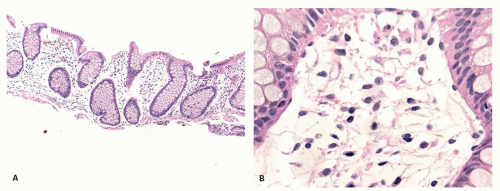 Figure 3-7. A: Large bowel mucosa with architectural distortion but an empty lamina propria. B: Detail showing almost entirely mesenchymal cells. Changes such as these can be seen in neonates and young children before the intestinal immune system has developed, in patients with immunologic disorders such as combined immunodeficiency disease, and also immediately following bone marrow transplantation before repopulation of the lamina propria has occurred. It can also be seen in some patients with inflammatory bowel disease following therapy and in remission. |
of the esophagus, the organism is present in the superficial necrotic debris and may invade the mucosa and occasionally extend through the bowel wall. In viral infections, inclusions tend to be scant and are frequently missed unless serial sections are carefully screened. The viral inclusions are commonly associated with mucosal erosions and ulcerations, often with minimal inflammation in the early stages.82 In AIDS, herpetic infections may be particularly intractable, especially herpetic proctitis, characterized by burrowing ulcers and destruction of the sphincter.81
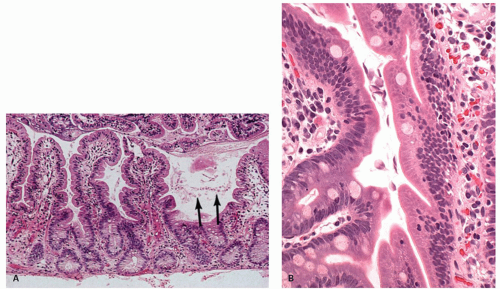 Figure 3-8. Intestinal giardiasis in a patient with common variable hypogammaglobulinemia. A: The jejunal mucosa is unremarkable. However, within the intestinal mucus are numerous giardial parasites (arrows). B: Detail of crypts showing numerous Giardia in the lumen, some probably attached to the epithelium. |
of age), lacks plasma cells in the atrophic mucosa, and lacks antibodies to intrinsic factor and parietal cells.76 Nodular lymphoid hyperplasia may be found in patients with CVID syndromes and selective IgA deficiency (Fig. 3-15).
Table 3-3 Incidence of Neoplasia in Immunodeficiency Disorders | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
inheritance can be discerned.76 Patients have panhypogammaglobulinemia and tend to present in one of two ways: either with recurrent infections, especially of the respiratory tract, or with chronic diarrhea and malabsorption.10, 74, 98 The intestinal symptoms are frequently due to giardiasis, although other parasites such as Cryptosporidium and strongyloidiasis as well as fungal overgrowth may also be responsible for the diarrhea and malabsorption.68, 69, 76, 80, 99 Other less common causes for chronic diarrhea are bacterial infections such as Campylobacter jejuni.100 These infections may sometimes be pathologically indistinguishable
from ulcerative colitis or result in mucosal fissuring and necrosis resembling Crohn’s disease.92, 101, 102 A third of these patients develop pernicious anemia and they may also develop a variety of other maladies, such as thyrotoxicosis, myxedema, arthritis, keratoconjunctivitis, splenomegaly, sarcoidosis, and amyloidosis secondary to infection.103 Most important, however, is the increased risk of GI tumors, especially gastric carcinoma in adults,88, 104 although lymphoma associated with nodular lymphoid hyperplasia as well as T-cell lymphoma unassociated with EBV viral infection have also been found.105, 106
Table 3-4 GI Manifestations of Primary Immunodeficiency Syndromes | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:
 Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
Gastrointestinal Manifestations of Extraintestinal Disorders and Systemic Disease
 Esophagus: Normal Structures, Developmental Abnormalities, and Miscellaneous Disorders
Esophagus: Normal Structures, Developmental Abnormalities, and Miscellaneous Disorders
 Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
Inflammatory Disorders of the Esophagus: Reflux and Nonreflux Types
 Small Bowel Mucosal Disease
Small Bowel Mucosal Disease
 Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
Stomach and Proximal Duodenum: Inflammatory and Miscellaneous Disorders
 Small and Large Bowel Polyps and Tumors
Small and Large Bowel Polyps and Tumors
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


