Imaging plays a critical role in the evaluation of patients with urolithiasis. It is essential for the diagnosis of stones and provides important information to aide in determining the appropriate treatment of renal or ureteral calculi. Imaging for urolithiasis has evolved over the past 30 years. Currently, noncontrast computed tomography remains the first-line imaging modality for the evaluation of patients with suspected urolithiasis. Proper imaging modality selection helps to minimize radiation exposure. Following the principles of As Low As Reasonably Achievable in the operating room can help reduce the amount of radiation patients are exposed to from fluoroscopy.
Key points
- •
Imaging is a key component in the evaluation and management of patients with urolithiasis.
- •
Non-contrast computed tomography is considered the first line imaging study for the diagnosis of urolithiasis and provides critical information for operative planning.
- •
Beyond diagnosis, imaging provides important information that allows urologists to determine the most appropriate treatment modality for the patient. This information includes the size, location, and in some cases composition of stones.
Introduction
Imaging is a key component in the evaluation and management of patients with urolithiasis. Imaging allows for the rapid and definitive diagnosis of stones. Beyond diagnosis, imaging provides important information that allows urologists to determine the most appropriate treatment modality for the patient. This information includes the size, location, and, in some cases, composition of stones.
Historically, plain abdominal radiography (KUB) and excretory radiography (IVP) have been considered the studies of choice for the evaluation of patients with stones. These modalities have been largely supplanted by noncontrast computed tomography of the abdomen and pelvis (NCCT). Ultrasound has also been used in place of traditional radiography. Magnetic resonance imaging (MRI) has a limited role in the evaluation of patients with suspected urolithiasis.
Patients with urolithiasis are at risk for significant radiation exposure from imaging studies. Most of the radiation comes from NCCT. Plain radiography also exposes stone patients to radiation. Once diagnosed with a stone, a significant number of patients will undergo surgical intervention. Fluoroscopy used during shock wave lithotripsy (SWL), ureteroscopy (URS), and percutaneous nephrolithotomy (PNL) contributes to the overall radiation exposure of patients with urolithiasis.
This article reviews currently available imaging modalities for the evaluation of urolithiasis. Methods to reduce radiation exposure to patients with stones are discussed as well.
Computed Tomography
Evaluation of renal colic
NCCT was first reported for the evaluation of urinary stones in the late 1970s. The initial indication for NCCT in the workup of urolithiasis was in diagnosing radiolucent stones. It was eventually demonstrated that NCCT had improved sensitivity for diagnosing ureteral stones in patients with flank pain compared with IVP. NCCT can be rapidly performed and does not require intravenous contrast. Unlike IVP, NCCT can identify stones of any composition, with the exception of stones formed by protease inhibitors, such as indinavir, which may not be visible on NCCT.
Currently, NCCT is considered the first-line imaging study for the evaluation of the patient with acute flank pain and a suspected stone. NCCT has a reported sensitivity of 95% to 98% and specificity of 96% to 98% for the diagnosis of a ureteral stone in a patient with acute flank pain ( Table 1 ). Besides identifying the stone, NCCT allows for the evaluation of the signs of obstruction associated with ureteral stones. In patients with ureteral stones, NCCT was able to identify hydroureter in 82.7% of cases, hydronephrosis in 80% of cases, periureteric edema in 59% of cases, and unilateral renal enlargement in 57.2% of cases.
| Imaging Technique | Sensitivity | Specificity |
|---|---|---|
| Noncontrast computed tomography | 95%–98% | 96%–98% |
| “Low-dose” CT | 97% | 95% |
| Ultrasound | ||
| Renal stones | 29%–81% | 82%–90% |
| Ureteral stones | 11%–93% | 87%–100% |
| Plain radiography | ||
| KUB | 45%–58% | 69%–77% |
| IVP | 85.2% | 90.4% |
| Magnetic resonance imaging | 93%–100% | 95%–100% |
When evaluating patients with acute flank pain, NCCT also has the ability to evaluate the rest of the abdominal and pelvic organs and possibly identify other causes of pain. In a series of 1000 consecutive NCCT performed for the evaluation of renal colic, an alternative diagnosis was made in 10.1% of the cases. In another report reviewing the results of 1500 NCCT performed for the evaluation of flank pain with a suspected stone, 24% of the patients had an alternative CT finding without a urinary calculus. In additional, another 7% had a completely negative CT. A urinary stone was identified in 69% of the patients, and of those patients with a stone, an additional pathologic condition was found in 47%.
Preoperative evaluation
Beyond the diagnosis of stones, NCCT is useful in the preoperative planning for the treatment of stones. Stone size and location are easily evaluated with NCCT. When planning SWL, the skin-to-stone distance can be determined on preoperative NCCT. This has been demonstrated to be an independent predictor of successful treatment with SWL. A skin-to-stone distance greater than or equal to 11 cm has been associated with worse stone-free outcomes for SWL when compared with skin-to-stone distances less than 11 cm. Prone NCCT can be useful for the preoperative evaluation for planning prone percutaneous nephrolithotomy (PNL). Prone NCCT can determine the anatomic relations of adjacent organs and the pleura with upper pole calyces. This information can help determine the feasibility and risk of complication of an upper pole puncture during prone PNL.
Stone composition
Determining the stone composition preoperatively can also aide in deciding the best surgical modality to treat the stone. NCCT can provide information to aide in the determination of different stone types. Hounsfield units or CT attenuation has been frequently used to help identify stone composition. Harder stone types typically have higher attenuations. Calcium oxalate and brushite stones have been shown to have the highest CT attenuations, averaging more than 1400 HU. Uric acid stones typically have the lowest CT attenuation, on average 409 HU. A number of reports have demonstrated that the efficacy of SWL decreases with increasing stone attenuation as measured on NCCT. One series found that the rate of success for stone fragmentation was significantly lower in stones with a CT attenuation greater than 1000 HU when compared with stones with lower attenuation. Another group reported a significantly higher effectiveness coefficient for SWL treating stones with attenuation less than 1200 HU versus those with greater than 1200 HU (80.4% vs 66.2%, P = .03). Finally, 2 reports have demonstrated that stone attenuation less than 900 HU is an independent predictor of SWL success.
Dual-energy NCCT is a novel technology that can be used to differentiate stones of different compositions more accurately. In an in vivo study, dual-energy NCCT was able to determine and differentiate stone compositions accurately, including stones of mixed composition. Dual-energy NCCT has also been very effective in determining uric acid stone composition.
Ultrasound
Ultrasound is commonly performed during the evaluation of urolithiasis. The main advantage ultrasound has over other imaging modalities such as NCCT is that it is performed without any radiation exposure to the patient. However, ultrasound is not as sensitive or specific for the detection of renal or ureteral stones. The reported sensitivity of ultrasound for diagnosing renal stones ranges from 29% to 81%. The specificity ranges from 82% to 90%. The sensitivity of ultrasound for the detection of ureteral stones in patients with acute renal colic ranges from 11% to 93% and the specificity ranges from 87% to 100%.
Evaluation of renal colic
The sensitivity of ultrasound for the identification of a ureteral stone in a patient with renal colic is less than NCCT; however, it still plays a large role in evaluating patients with renal colic. Ultrasound, like NCCT, can be used to evaluate other abdominal or pelvic organs while concurrently imaging the urinary tract. This allows for identification of alternative diagnoses when evaluating for renal colic. One study comparing the sensitivity of ultrasound and NCCT for the diagnosis of a ureteral stone in patients with renal colic found that ultrasound had a significantly lower sensitivity compared with NCCT, 61% versus 96% ( P = .02). However, the sensitivity for ultrasound in determining any cause for the patient’s symptoms, including hydronephrosis, stones, or appendicitis, was 85%. Another study comparing ultrasound and NCCT for the evaluation of renal colic found a 93% sensitivity for the diagnosis of a ureteral stone with ultrasound. In 6 of the 62 patients included in this study, ultrasound was able to find an alternative diagnosis: appendicitis, cholecystitis, cholelithiasis, adnexal mass, and torsed ovary.
When patients with renal colic are diagnosed with a distal ureteral stone with an NCCT, ultrasound can be effective at identifying the stone in the distal ureter during follow-up. One prospective study looked at the utility of ultrasound to follow up patients diagnosed with distal ureteral stones on an initial NCCT. After their initial diagnosis, during follow-up the patients were imaged with ultrasound in addition to either repeat NCCT or radiography. The sensitivity of ultrasound on follow-up was 94.3% and the specificity was 99.1%.
Color Doppler ultrasound can be useful to improve the ability of ultrasound to detect ureteral stones. The “twinkling sign” on Doppler ultrasound appears as random color encoding in the area behind the stone where shadowing would be seen in traditional B-mode ultrasound. Doppler ultrasound using the “twinkling sign” has been shown to detect a higher percentage of stones than traditional gray-scale ultrasonography, 97% versus 66%.
Evaluation for obstruction
In patients with renal colic, ultrasound is excellent at identifying signs of ureteral obstruction. The sensitivity and specificity of ultrasound for the diagnosis of obstruction have been reported to be as high as 100%. In 1 study looking at ultrasound for the evaluation of patients with confirmed renal colic, hydronephrosis was identified in 95% of cases, ureteral dilation in 89% of cases, and perirenal fluid in 23% of cases.
In addition to these signs of obstruction, the resistive index (RI) is a measure on color Doppler ultrasound that can improve the detection of ureteral obstruction in patients with renal colic. Ultrasound-determined RI has been shown to have a sensitivity of 88% and a specificity of 98% for ureteral obstruction, using IVP as the standard. In this report, the RI in the obstructed kidneys were significantly greater than the RI in nonobstructed kidneys, 0.73 versus 0.64 ( P <.001). In a prospective study, Doppler ultrasound with RI performed equally well when compared with NCCT for the detection of ureteral obstruction. With IVP being the standard, the sensitivity and specificity for NCCT were 96% and 96% compared with 90% and 100% for Doppler ultrasound. Using an RI of 0.70 and a 10% difference in RI between kidneys as diagnostic of obstruction improves the sensitivity and specificity of ultrasound for the diagnosis of ureteral obstruction from 94.8% and 55.5% to 98.9% and 90.9%. Doppler ultrasound can also identify ureteral jets, which can further aide in ruling out obstruction.
Limitations of ultrasound in the evaluation of urolithiasis
Ultrasound has limitations in the evaluation of urolithiasis and these are to stone location, size, and patient size. Ultrasound is not as sensitive at identifying stones in the ureter as it is in identifying stones in the kidney. One study evaluated 228 patients who underwent ultrasound for renal colic and suspected renal colic before ureteroscopy and found the sensitivity of ultrasound was 86.4% for identifying ureteral stones. Patients in whom ultrasound failed to diagnose the stone had significantly smaller mean stone size (4 mm vs 6 mm, P <.001). In addition to being less sensitive at identifying smaller stones, ultrasound has been shown to overestimate stone size compared with NCCT. In 1 report, ultrasound overestimated stone size by nearly 2 mm compared with NCCT. The mean stone size on NCCT was 7.4 ± 4 mm versus 9.2 ± 5 mm on ultrasound ( P = .018). Patient body habitus and body mass index (BMI) are other factors that can influence the accuracy of ultrasound. As the skin-to-stone distance increases, the discordance between ultrasound and NCCT for the measurement of stone size increases. The ability of ultrasound to detect stones has been shown to be lower in patients with higher BMI.
Plain Radiography
Plain radiography of the abdomen/pelvis
Historically, KUB was the imaging modality of choice for the evaluation of urolithiasis. This was because most stones contained calcium and therefore would be expected to be visible on KUB. However, compared with NCCT and ultrasound, the sensitivity and specificity of KUB for detecting stones are poor. The sensitivity of KUB is reported to be 45 to 58%; the specificity is reported to be 69 to 77%. There are a number of factors that contribute to the reduced sensitivity and specificity of KUB, such as overlying bowel gas, extrarenal and extra-ureteral calcifications, and patient body habitus.
The use of tomography can improve the diagnostic accuracy of KUB for the evaluation of nephrolithiasis. In 1 study evaluating KUB versus KUB with tomograms, 46% of patients had additional stones identified on tomograms. In 8% of patients, stones were only seen on tomograms. The use of tomograms increases the amount of radiation the patient is exposed to. The effective doses for a KUB and each tomogram have been estimated to be 0.67 mSv and 1.1 mSv, respectively. Therefore, if a KUB is performed with 3 tomograms, the total radiation exposure would be 3.97 mSv, greater than a low-dose NCCT.
KUB with ultrasound
KUB is useful as an adjunct to ultrasound in the evaluation of patients with renal colic. The sensitivity of ultrasound combined with KUB for the diagnosis of a ureteral calculus in a patient with renal colic has been reported to be as high as 96% with a specificity of 91%. When performed together, it is recommended that KUB be performed first to identify calcifications. Ultrasound can then be used to confirm that these calcifications are in the urinary tract and therefore are stones.
Preoperative evaluation
KUB is useful in the preoperative evaluation before SWL. It can determine if a stone is radio-opaque and thereby seen with fluoroscopy. Obtaining a KUB can change the decision on how a stone is managed. One study reported that when a KUB is obtained after NCCT, the surgical management was changed in 17 of 100 patients based on information from the KUB. An NCCT scout image is not as sensitive for identifying stones compared with a KUB. Therefore, scout images from NCCT cannot be used as a surrogate for a KUB, and if SWL using fluoroscopy is planned, a KUB should be obtained preoperatively to determine if the stone will be visible on fluoroscopy during SWL.
Intravenous Pyelography
Before the advent of NCCT, IVP was considered the standard imaging technique for the evaluation of patients with renal colic. Currently, NCCT has largely supplanted IVP because of its superior sensitivity for detecting stones in these patients. In a prospective randomized trial comparing NCCT with IVP for the evaluation of acute flank pain, NCCT was demonstrated to have a sensitivity and specificity of 94.1% and 94.2% for identifying a stone compared with a sensitivity and specificity of 85.2% and 90.4% for IVP.
There are still some advantages of IVP in the evaluation of patients with urolithiasis. Because it is performed with contrast, IVP can provide information about renal function and whether a kidney is obstructed. Delayed images can be useful in evaluating ureteral anatomy for filling defects or strictures. It also provides detailed pelvicalyceal anatomy, which can be useful in planning surgical interventions, especially in those individuals with urinary tract anomalies. However, for these indications, IVP has largely been supplanted by CT with intravenous contrast or CT urograms.
Magnetic Resonance Imaging
There are limited indications for the use of MRI in the evaluation of urolithiasis. Although stones cannot be directly visualized using MRI, when evaluating patients with renal colic, MRI can detect signs of obstruction and can evaluate for alternative diagnoses. A number of different techniques and sequences have been reported for the evaluation of stones. The most common technique is to evaluate the T2-weighted images and assess for signs of obstruction or look for filling defects, which may be stones. Using T2-weighted images, the findings of perirenal fluid and ureteral dilation had a sensitivity and specificity of 93% and 95% for the diagnosis of ureteral calculi in patients with renal colic. Another group reported using a 3-dimensional fast low-angle shot (3D FLASH) sequence that requires the administration of gadolinium. The sensitivity and specificity for the 3D FLASH sequence was 96.2% to 100% and 100% for the diagnosis of a ureteral stone. The 3D FLASH sequence combined with T2-weighted images has been shown to be as sensitive and specific for the diagnosis of ureteral stones as NCCT. The addition of gadolinium for the 3D FLASH sequence can aide in the determination of stone size on MRI.
New Technology
Digital tomosynthesis
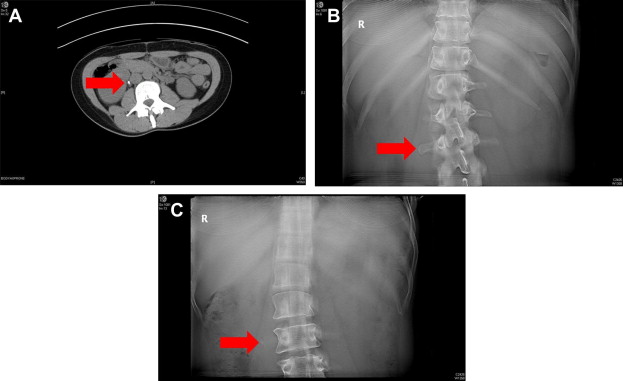
Digital tomosynthesis (DT) is a new imaging technology similar to KUB with tomograms. When DT is performed, a scout KUB is taken and then a single tomographic sweep over approximately 60° arc is done. A digital flat-panel detector records the data from the sweep and then software reconstructs the information to provide high-resolution “slice” or coronal images at varying depths ( Fig. 1 ). This reconstruction removes overlying structures such as bowel gas from slices, improving the resolution and visualization of stones. It also provides depth information. The depth information is useful in differentiating a calcification in the ureter versus an overlying transverse process from the spine (see Fig. 1 ).
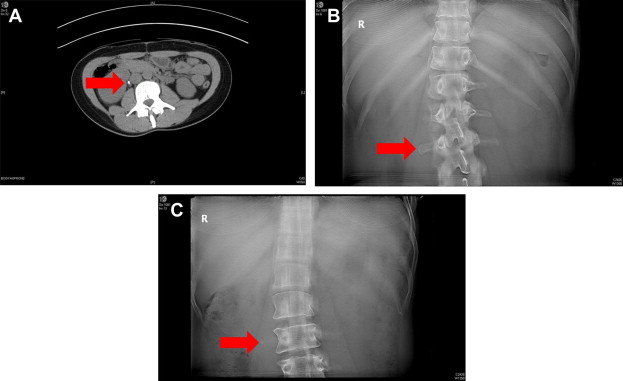
There have been reports of the use of DT for the evaluation of urolithiasis. In 1 report, DT was compared with KUB with an additional plain film of the pelvis. All patients underwent DT, KUB with the additional image of the pelvis, and NCCT, which was used as the standard. DT was superior to KUB for identifying intrarenal stones. The technology for DT can be used to perform an IVP, improving the image quality. Two uroradiologists reviewed both traditional IVP and IVP performed with DT. They evaluated the subjective diagnostic quality and found that 95.5% of the IVP with DT were of diagnostic quality versus 46.5% of the traditional IVPs. In addition, the dose of radiation was lower for the IVP with DT and they took less time. The dose of radiation from DT has been shown to be lower than that of a “low-dose” NCCT.
Introduction
Imaging is a key component in the evaluation and management of patients with urolithiasis. Imaging allows for the rapid and definitive diagnosis of stones. Beyond diagnosis, imaging provides important information that allows urologists to determine the most appropriate treatment modality for the patient. This information includes the size, location, and, in some cases, composition of stones.
Historically, plain abdominal radiography (KUB) and excretory radiography (IVP) have been considered the studies of choice for the evaluation of patients with stones. These modalities have been largely supplanted by noncontrast computed tomography of the abdomen and pelvis (NCCT). Ultrasound has also been used in place of traditional radiography. Magnetic resonance imaging (MRI) has a limited role in the evaluation of patients with suspected urolithiasis.
Patients with urolithiasis are at risk for significant radiation exposure from imaging studies. Most of the radiation comes from NCCT. Plain radiography also exposes stone patients to radiation. Once diagnosed with a stone, a significant number of patients will undergo surgical intervention. Fluoroscopy used during shock wave lithotripsy (SWL), ureteroscopy (URS), and percutaneous nephrolithotomy (PNL) contributes to the overall radiation exposure of patients with urolithiasis.
This article reviews currently available imaging modalities for the evaluation of urolithiasis. Methods to reduce radiation exposure to patients with stones are discussed as well.
Computed Tomography
Evaluation of renal colic
NCCT was first reported for the evaluation of urinary stones in the late 1970s. The initial indication for NCCT in the workup of urolithiasis was in diagnosing radiolucent stones. It was eventually demonstrated that NCCT had improved sensitivity for diagnosing ureteral stones in patients with flank pain compared with IVP. NCCT can be rapidly performed and does not require intravenous contrast. Unlike IVP, NCCT can identify stones of any composition, with the exception of stones formed by protease inhibitors, such as indinavir, which may not be visible on NCCT.
Currently, NCCT is considered the first-line imaging study for the evaluation of the patient with acute flank pain and a suspected stone. NCCT has a reported sensitivity of 95% to 98% and specificity of 96% to 98% for the diagnosis of a ureteral stone in a patient with acute flank pain ( Table 1 ). Besides identifying the stone, NCCT allows for the evaluation of the signs of obstruction associated with ureteral stones. In patients with ureteral stones, NCCT was able to identify hydroureter in 82.7% of cases, hydronephrosis in 80% of cases, periureteric edema in 59% of cases, and unilateral renal enlargement in 57.2% of cases.
| Imaging Technique | Sensitivity | Specificity |
|---|---|---|
| Noncontrast computed tomography | 95%–98% | 96%–98% |
| “Low-dose” CT | 97% | 95% |
| Ultrasound | ||
| Renal stones | 29%–81% | 82%–90% |
| Ureteral stones | 11%–93% | 87%–100% |
| Plain radiography | ||
| KUB | 45%–58% | 69%–77% |
| IVP | 85.2% | 90.4% |
| Magnetic resonance imaging | 93%–100% | 95%–100% |
When evaluating patients with acute flank pain, NCCT also has the ability to evaluate the rest of the abdominal and pelvic organs and possibly identify other causes of pain. In a series of 1000 consecutive NCCT performed for the evaluation of renal colic, an alternative diagnosis was made in 10.1% of the cases. In another report reviewing the results of 1500 NCCT performed for the evaluation of flank pain with a suspected stone, 24% of the patients had an alternative CT finding without a urinary calculus. In additional, another 7% had a completely negative CT. A urinary stone was identified in 69% of the patients, and of those patients with a stone, an additional pathologic condition was found in 47%.
Preoperative evaluation
Beyond the diagnosis of stones, NCCT is useful in the preoperative planning for the treatment of stones. Stone size and location are easily evaluated with NCCT. When planning SWL, the skin-to-stone distance can be determined on preoperative NCCT. This has been demonstrated to be an independent predictor of successful treatment with SWL. A skin-to-stone distance greater than or equal to 11 cm has been associated with worse stone-free outcomes for SWL when compared with skin-to-stone distances less than 11 cm. Prone NCCT can be useful for the preoperative evaluation for planning prone percutaneous nephrolithotomy (PNL). Prone NCCT can determine the anatomic relations of adjacent organs and the pleura with upper pole calyces. This information can help determine the feasibility and risk of complication of an upper pole puncture during prone PNL.
Stone composition
Determining the stone composition preoperatively can also aide in deciding the best surgical modality to treat the stone. NCCT can provide information to aide in the determination of different stone types. Hounsfield units or CT attenuation has been frequently used to help identify stone composition. Harder stone types typically have higher attenuations. Calcium oxalate and brushite stones have been shown to have the highest CT attenuations, averaging more than 1400 HU. Uric acid stones typically have the lowest CT attenuation, on average 409 HU. A number of reports have demonstrated that the efficacy of SWL decreases with increasing stone attenuation as measured on NCCT. One series found that the rate of success for stone fragmentation was significantly lower in stones with a CT attenuation greater than 1000 HU when compared with stones with lower attenuation. Another group reported a significantly higher effectiveness coefficient for SWL treating stones with attenuation less than 1200 HU versus those with greater than 1200 HU (80.4% vs 66.2%, P = .03). Finally, 2 reports have demonstrated that stone attenuation less than 900 HU is an independent predictor of SWL success.
Dual-energy NCCT is a novel technology that can be used to differentiate stones of different compositions more accurately. In an in vivo study, dual-energy NCCT was able to determine and differentiate stone compositions accurately, including stones of mixed composition. Dual-energy NCCT has also been very effective in determining uric acid stone composition.
Ultrasound
Ultrasound is commonly performed during the evaluation of urolithiasis. The main advantage ultrasound has over other imaging modalities such as NCCT is that it is performed without any radiation exposure to the patient. However, ultrasound is not as sensitive or specific for the detection of renal or ureteral stones. The reported sensitivity of ultrasound for diagnosing renal stones ranges from 29% to 81%. The specificity ranges from 82% to 90%. The sensitivity of ultrasound for the detection of ureteral stones in patients with acute renal colic ranges from 11% to 93% and the specificity ranges from 87% to 100%.
Evaluation of renal colic
The sensitivity of ultrasound for the identification of a ureteral stone in a patient with renal colic is less than NCCT; however, it still plays a large role in evaluating patients with renal colic. Ultrasound, like NCCT, can be used to evaluate other abdominal or pelvic organs while concurrently imaging the urinary tract. This allows for identification of alternative diagnoses when evaluating for renal colic. One study comparing the sensitivity of ultrasound and NCCT for the diagnosis of a ureteral stone in patients with renal colic found that ultrasound had a significantly lower sensitivity compared with NCCT, 61% versus 96% ( P = .02). However, the sensitivity for ultrasound in determining any cause for the patient’s symptoms, including hydronephrosis, stones, or appendicitis, was 85%. Another study comparing ultrasound and NCCT for the evaluation of renal colic found a 93% sensitivity for the diagnosis of a ureteral stone with ultrasound. In 6 of the 62 patients included in this study, ultrasound was able to find an alternative diagnosis: appendicitis, cholecystitis, cholelithiasis, adnexal mass, and torsed ovary.
When patients with renal colic are diagnosed with a distal ureteral stone with an NCCT, ultrasound can be effective at identifying the stone in the distal ureter during follow-up. One prospective study looked at the utility of ultrasound to follow up patients diagnosed with distal ureteral stones on an initial NCCT. After their initial diagnosis, during follow-up the patients were imaged with ultrasound in addition to either repeat NCCT or radiography. The sensitivity of ultrasound on follow-up was 94.3% and the specificity was 99.1%.
Color Doppler ultrasound can be useful to improve the ability of ultrasound to detect ureteral stones. The “twinkling sign” on Doppler ultrasound appears as random color encoding in the area behind the stone where shadowing would be seen in traditional B-mode ultrasound. Doppler ultrasound using the “twinkling sign” has been shown to detect a higher percentage of stones than traditional gray-scale ultrasonography, 97% versus 66%.
Evaluation for obstruction
In patients with renal colic, ultrasound is excellent at identifying signs of ureteral obstruction. The sensitivity and specificity of ultrasound for the diagnosis of obstruction have been reported to be as high as 100%. In 1 study looking at ultrasound for the evaluation of patients with confirmed renal colic, hydronephrosis was identified in 95% of cases, ureteral dilation in 89% of cases, and perirenal fluid in 23% of cases.
In addition to these signs of obstruction, the resistive index (RI) is a measure on color Doppler ultrasound that can improve the detection of ureteral obstruction in patients with renal colic. Ultrasound-determined RI has been shown to have a sensitivity of 88% and a specificity of 98% for ureteral obstruction, using IVP as the standard. In this report, the RI in the obstructed kidneys were significantly greater than the RI in nonobstructed kidneys, 0.73 versus 0.64 ( P <.001). In a prospective study, Doppler ultrasound with RI performed equally well when compared with NCCT for the detection of ureteral obstruction. With IVP being the standard, the sensitivity and specificity for NCCT were 96% and 96% compared with 90% and 100% for Doppler ultrasound. Using an RI of 0.70 and a 10% difference in RI between kidneys as diagnostic of obstruction improves the sensitivity and specificity of ultrasound for the diagnosis of ureteral obstruction from 94.8% and 55.5% to 98.9% and 90.9%. Doppler ultrasound can also identify ureteral jets, which can further aide in ruling out obstruction.
Limitations of ultrasound in the evaluation of urolithiasis
Ultrasound has limitations in the evaluation of urolithiasis and these are to stone location, size, and patient size. Ultrasound is not as sensitive at identifying stones in the ureter as it is in identifying stones in the kidney. One study evaluated 228 patients who underwent ultrasound for renal colic and suspected renal colic before ureteroscopy and found the sensitivity of ultrasound was 86.4% for identifying ureteral stones. Patients in whom ultrasound failed to diagnose the stone had significantly smaller mean stone size (4 mm vs 6 mm, P <.001). In addition to being less sensitive at identifying smaller stones, ultrasound has been shown to overestimate stone size compared with NCCT. In 1 report, ultrasound overestimated stone size by nearly 2 mm compared with NCCT. The mean stone size on NCCT was 7.4 ± 4 mm versus 9.2 ± 5 mm on ultrasound ( P = .018). Patient body habitus and body mass index (BMI) are other factors that can influence the accuracy of ultrasound. As the skin-to-stone distance increases, the discordance between ultrasound and NCCT for the measurement of stone size increases. The ability of ultrasound to detect stones has been shown to be lower in patients with higher BMI.
Plain Radiography
Plain radiography of the abdomen/pelvis
Historically, KUB was the imaging modality of choice for the evaluation of urolithiasis. This was because most stones contained calcium and therefore would be expected to be visible on KUB. However, compared with NCCT and ultrasound, the sensitivity and specificity of KUB for detecting stones are poor. The sensitivity of KUB is reported to be 45 to 58%; the specificity is reported to be 69 to 77%. There are a number of factors that contribute to the reduced sensitivity and specificity of KUB, such as overlying bowel gas, extrarenal and extra-ureteral calcifications, and patient body habitus.
The use of tomography can improve the diagnostic accuracy of KUB for the evaluation of nephrolithiasis. In 1 study evaluating KUB versus KUB with tomograms, 46% of patients had additional stones identified on tomograms. In 8% of patients, stones were only seen on tomograms. The use of tomograms increases the amount of radiation the patient is exposed to. The effective doses for a KUB and each tomogram have been estimated to be 0.67 mSv and 1.1 mSv, respectively. Therefore, if a KUB is performed with 3 tomograms, the total radiation exposure would be 3.97 mSv, greater than a low-dose NCCT.
KUB with ultrasound
KUB is useful as an adjunct to ultrasound in the evaluation of patients with renal colic. The sensitivity of ultrasound combined with KUB for the diagnosis of a ureteral calculus in a patient with renal colic has been reported to be as high as 96% with a specificity of 91%. When performed together, it is recommended that KUB be performed first to identify calcifications. Ultrasound can then be used to confirm that these calcifications are in the urinary tract and therefore are stones.
Preoperative evaluation
KUB is useful in the preoperative evaluation before SWL. It can determine if a stone is radio-opaque and thereby seen with fluoroscopy. Obtaining a KUB can change the decision on how a stone is managed. One study reported that when a KUB is obtained after NCCT, the surgical management was changed in 17 of 100 patients based on information from the KUB. An NCCT scout image is not as sensitive for identifying stones compared with a KUB. Therefore, scout images from NCCT cannot be used as a surrogate for a KUB, and if SWL using fluoroscopy is planned, a KUB should be obtained preoperatively to determine if the stone will be visible on fluoroscopy during SWL.
Intravenous Pyelography
Before the advent of NCCT, IVP was considered the standard imaging technique for the evaluation of patients with renal colic. Currently, NCCT has largely supplanted IVP because of its superior sensitivity for detecting stones in these patients. In a prospective randomized trial comparing NCCT with IVP for the evaluation of acute flank pain, NCCT was demonstrated to have a sensitivity and specificity of 94.1% and 94.2% for identifying a stone compared with a sensitivity and specificity of 85.2% and 90.4% for IVP.
There are still some advantages of IVP in the evaluation of patients with urolithiasis. Because it is performed with contrast, IVP can provide information about renal function and whether a kidney is obstructed. Delayed images can be useful in evaluating ureteral anatomy for filling defects or strictures. It also provides detailed pelvicalyceal anatomy, which can be useful in planning surgical interventions, especially in those individuals with urinary tract anomalies. However, for these indications, IVP has largely been supplanted by CT with intravenous contrast or CT urograms.
Magnetic Resonance Imaging
There are limited indications for the use of MRI in the evaluation of urolithiasis. Although stones cannot be directly visualized using MRI, when evaluating patients with renal colic, MRI can detect signs of obstruction and can evaluate for alternative diagnoses. A number of different techniques and sequences have been reported for the evaluation of stones. The most common technique is to evaluate the T2-weighted images and assess for signs of obstruction or look for filling defects, which may be stones. Using T2-weighted images, the findings of perirenal fluid and ureteral dilation had a sensitivity and specificity of 93% and 95% for the diagnosis of ureteral calculi in patients with renal colic. Another group reported using a 3-dimensional fast low-angle shot (3D FLASH) sequence that requires the administration of gadolinium. The sensitivity and specificity for the 3D FLASH sequence was 96.2% to 100% and 100% for the diagnosis of a ureteral stone. The 3D FLASH sequence combined with T2-weighted images has been shown to be as sensitive and specific for the diagnosis of ureteral stones as NCCT. The addition of gadolinium for the 3D FLASH sequence can aide in the determination of stone size on MRI.
New Technology
Digital tomosynthesis
Digital tomosynthesis (DT) is a new imaging technology similar to KUB with tomograms. When DT is performed, a scout KUB is taken and then a single tomographic sweep over approximately 60° arc is done. A digital flat-panel detector records the data from the sweep and then software reconstructs the information to provide high-resolution “slice” or coronal images at varying depths ( Fig. 1 ). This reconstruction removes overlying structures such as bowel gas from slices, improving the resolution and visualization of stones. It also provides depth information. The depth information is useful in differentiating a calcification in the ureter versus an overlying transverse process from the spine (see Fig. 1 ).
Related posts:
 Metabolic Evaluation of First-time and Recurrent Stone Formers
New Insights Into the Pathogenesis of Renal Calculi
Diet and Alternative Therapies in the Management of Stone Disease
The Emerging Role of Robotics and Laparoscopy in Stone Disease
Impact of Stone Disease
Pharmacologic Treatment of Kidney Stone Disease
Metabolic Evaluation of First-time and Recurrent Stone Formers
New Insights Into the Pathogenesis of Renal Calculi
Diet and Alternative Therapies in the Management of Stone Disease
The Emerging Role of Robotics and Laparoscopy in Stone Disease
Impact of Stone Disease
Pharmacologic Treatment of Kidney Stone Disease
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


