Fig. 10.1
Positions of surgeons. CS chief abdominal surgeon, AS: assistant surgeon, CA camera surgeon, PS perineal surgeon, SNA scrub nurse for abdominal part, SNP scrub nurse for perineal part
Fig. 10.2
Port sites for the hybrid NOTES colectomy
The Lateral to Medial Approach
After pneumoperitoneum is established, a thorough diagnostic laparoscopy is first performed to localize the tumor and to look for any peritoneal deposits and ascitic fluid. In female, if the uterus is in the way, the uterus can be slung up by sutures through the abdominal wall to improve exposure. The operation is started with a lateral first approach (our preference) along the white line of Toldt. The left-sided colon is mobilized and the left ureter is identified and protected. The assistant surgeon provides counter-traction of the colon by holding a cotton tape which was passed through the sigmoid mesentery (Fig. 10.3). During medial dissection, the assistant surgeon retracts the sigmoid colon towards the abdominal wall to tent up the mesentery. A mesenteric window is made in the sigmoid mesocolon and dissection is carried out upwards. The inferior mesenteric vessels are then dissected out and divided by vascular staplers or between endo-clips
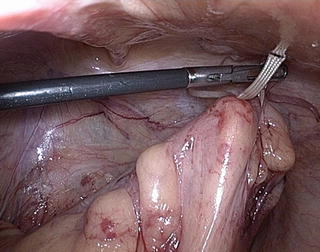
Fig. 10.3
The assistant surgeon provides counter-traction of the colon by holding a cotton tape
Mobilization of the Rectum
Presacral dissection is carried out distal to the tumor. Attention should be paid to preserve the hypogastric nerves. The distal level of transection should be 5 cm distal to the tumor. The mesentery at the intended level of transection is divided. The abdominal surgeon uses a pair of atraumatic laparoscopic bowel forceps to occlude the bowel just proximal to the “nude” rectal tube; the perineal surgeon then quickly carries out distal cytocidal rectal lavage with povidone-iodine solution so as to reduce the risk of tumor seeding and peritoneal contamination. Non-cutting endo-staplers are applied at the chosen level distal to the tumors to exclude the tumor distally (Figs. 10.4 and 10.5). An alternate way to exclude the tumor is by tying the colon with a cotton tape.


Fig. 10.4
Non-cutting endo-staplers are applied at the chosen level distal to the tumors to exclude the tumor distally
Fig. 10.5
Non-cutting endo-staplers are applied at the chosen level distal to the tumors to exclude the tumor distally
Insertion of the TEO Device and the Passage of the Anvil
Next the perineal surgeon inserts the TEO device (Fig. 10.6) through the anus and it is fixed externally. The abdominal surgeon then divides the rectum just distal to the staple line or the cotton tape by energy device until the rectal stump is opened (Fig. 10.7). The TEO device helps to maintain pneumoperitoneum by simultaneously insufflating the rectum with carbon dioxide. The rectal stump is kept opened by grasping the edge of the rectal stump on either side using atraumatic forceps (Fig. 10.8). The detachable anvil (with the spike anchored on it) of a 31-mm circular stapler (DST Series EEA; AutoSuture, Norwalk, CT) is then passed via the TEO device and manipulated into the peritoneal cavity by the perineal surgeon under direct vision (Fig. 10.9).

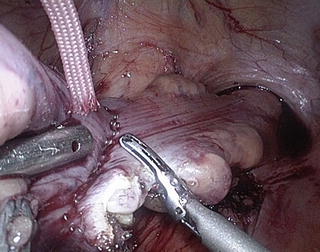
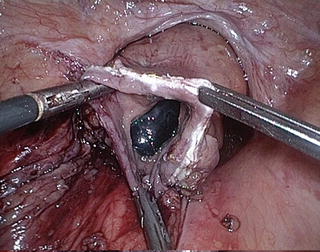
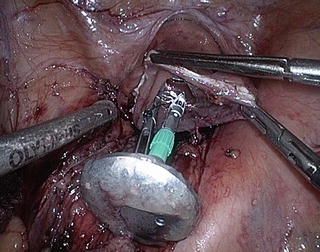
Fig. 10.6
The TEO device inserted through the anus
Fig. 10.7
The rectum is divided just distal to the staple line
Fig. 10.8
The rectum is kept opened by grasping the edge of the rectal stump using atraumatic forceps
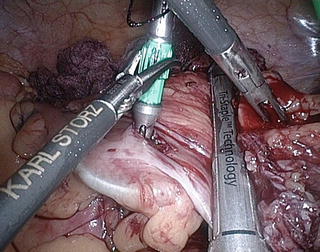
Fig. 10.9
The anvil is passed through the TEO device into the peritoneal cavity
Proximal Transection and Specimen Retrieval
Next the colonic mesentery at the intended level of proximal bowel division is divided. The abdominal surgeon fires a non-cutting endo-stapler at a point about 5 cm distal to the intended line of bowel division to exclude the colon from the tumor below. Again, a cotton tape is an alternative of a non-cutting endo-stapler. A colotomy is then made immediately proximal to the proximal staple line or cotton tape, and the anvil is gently inserted through the colotomy into the proximal colon. The abdominal surgeon then carefully manipulates the anvil such that the spike is delivered through the anti-mesenteric side of the colon, proximal to the intended line of division; the spike can then be easily removed via the 5–12 mm port in the right iliac fossa. The colon is finally transected proximal to the colotomy site by a cutting endo-stapler. The specimen now becomes free (Fig. 10.10). Under laparoscopic and endoscopic guidance, the resected specimen is slowly extracted through the TEO device (Fig. 10.11). The TEO device serves as a stable conduit against tumor seeding and protects the rectum and anus from injury during specimen retrieval. This technique avoids the need to create a mini-laparotomy wound for specimen retrieval.
 Single Incision Laparoscopic Right Colectomy
Single Incision Laparoscopic Right Colectomy
 Tricks and Routes to Success
Tricks and Routes to Success
 Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
 Robotic Single Port Colorectal Surgery
Robotic Single Port Colorectal Surgery
 Platforms and Instruments (Principles of Single-Incision Laparoscopic Colorectal Surgery, Available Platforms and Instruments)
Platforms and Instruments (Principles of Single-Incision Laparoscopic Colorectal Surgery, Available Platforms and Instruments)
 Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks




Related posts:
Single Incision Laparoscopic Right Colectomy
Tricks and Routes to Success
Transanal Endoluminal Total Mesorectal Resection (TETMR) by Transanal Endoscopic Microsurgery (TEM)
Robotic Single Port Colorectal Surgery
Platforms and Instruments (Principles of Single-Incision Laparoscopic Colorectal Surgery, Available Platforms and Instruments)
Local Excision (LE) for Low Rectal Cancer (RC): From Mucosectomy to Endolumen Loco-Regional Resection (ELRR)—Tips and Tricks
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
