How the Spine Works
Overview of the spinal column
The human backbone, or spinal column, is made up of 33 individual bones. Each bone is called a vertebra (see fig. 1.1) and the vertebrae are formed into five groups depending on their location and to a lesser degree their function. In the neck the bones, called cervical vertebrae, are delicate but highly mobile, enabling you to turn your head fully. Each vertebra is numbered using a code which indicates its group and position. Cervical vertebrae numbers begin with ‘C’, thoracic ‘T’, lumbar ‘L’ and sacral ‘S’. So, for example, the second cervical vertebra counting down from the head is C2, and the fourth is C4. The last lumber vertebra is L5 (rather than L1) because the numbering system begins at the head each time.
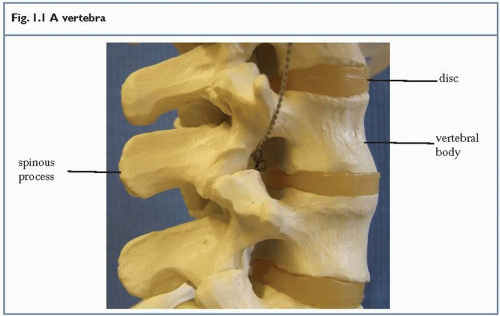 Fig. 1.1 A vertebra |
Keypoint
Vertebrae are numbered from the head down, with C1 just below the head and C7 between the shoulders.
The cervical region is subdivided into two functional parts. The upper portion directly below the head is called the sub-occipital region (the occiput being the lower back portion of the skull). The C1 and C2 bones make up this region and these two bones are intimately involved in skull movements, especially nodding actions. The lower portion of the neck is called the lower cervical region and takes in the bones C3 to C7. This region is more involved with twisting (rotation) and side bending (lateral flexion) actions.
In the chest region the bones are called ‘thoracic vertebrae’ and these bones connect to the ribs. There are two joints linking the thoracic vertebrae to the ribs: the costovertebral (CV) joint between the vertebral body and the rib, and the costotransverse (CT) joint between the transverse process at the side of the vertebra and the rib angle, where the rib curves to form the drum of the chest (see fig. 1.2).
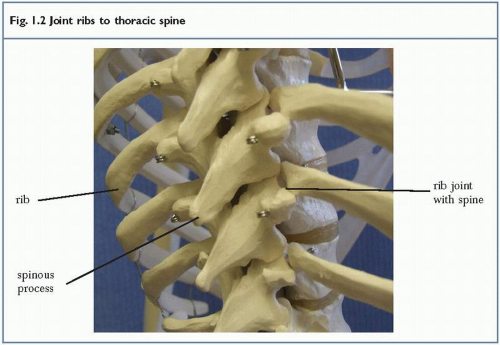 Fig. 1.2 Joint ribs to thoracic spine |
When looking at someone’s back, the spinous processes are in the middle, forming a straight column of bumps. The CV joint is about two finger breadths to the side, lying in the furrow of the back. The CT joint is about three finger breadths to the side, covered by the large erector spinae muscles.
Keypoint
In the thoracic spine, the spinous process is in the centre of the back, the costovertebral joint slightly out to the side, and the costotransverse joint further out still.
In the lower spine the spinal bones are called lumbar vertebrae. These are large, strong bones covered with powerful muscles. They do not attach to the ribs but their movements are intimately linked to those of the pelvis. The upper portion of the lumbar spine, L1 and L2 move with the thoracic spine, especially during shoulder blade and ribcage movements. The lower lumbar vertebrae, L3/4/5, move closely with the pelvis so that this combined region is often referred to as the lumbo-pelvis.
Below the lumbar vertebrae are the remnants of our tail. The sacrum is a triangularshaped bone which attaches at the sides to the pelvis, while the coccyx (see fig. 1.3) forms a thin, pointed tip to the end of the spine. Both of these regions are important in terms of injury, especially during pregnancy and childbirth. The joint between the sacrum and the pelvis (sacroiliac joint) is filled with fibrous material and normally gives little movement (see fig. 1.4). During childbirth, however, the fibrous material softens and the joint moves to allow the pelvis to expand to facilitate childbirth. This motion can inflame the joint and lead to changes in its alignment. The coccyx again becomes more mobile in this period and can give problems. In addition, in the lean individual, the coccyx is easily damaged by sitting or falling backwards directly onto a hard floor.
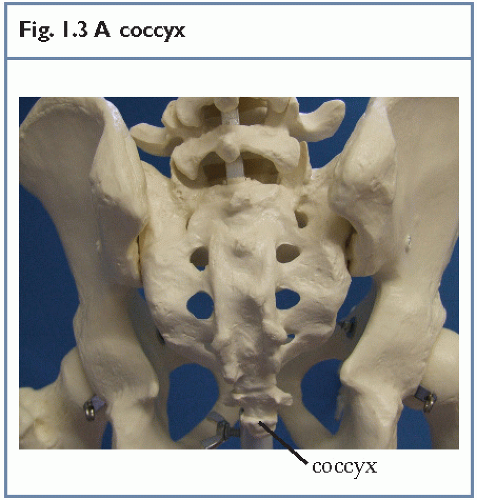 Fig. 1.3 A coccyx |
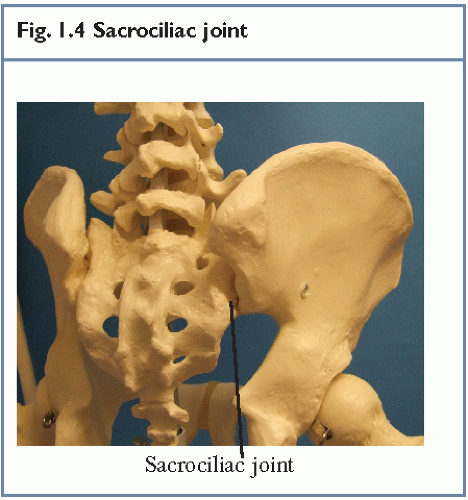 Fig. 1.4 Sacrociliac joint |
Keypoint
The sacrociliac joint joins the sacrum to the pelvis. It is often painful during pregnancy and following childbirth.
Spinal curves
Although the spinal vertebrae stand one on top of each other, the column they make is not straight. Instead, the spine forms an ‘S’ curve. There are two inward curves in the lower back and neck, while the thoracic spine curves gently outwards. These curves are not present at birth but begin to develop in early childhood.
In the early years of life, a baby’s spine is rounded, and we call this rounded shape the primary spinal curve (see fig. 1.6a). As the baby starts to lie on its front and lift its head up, the neck curve starts to form (see fig. 1.6b). It is not until a baby stands up that the curve in the lower back is formed (see fig. 1.6c). Because the neck and lower back curves form later, they are called secondary spinal curves.
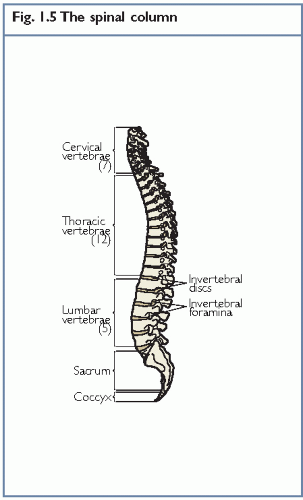 Fig. 1.5 The spinal column |
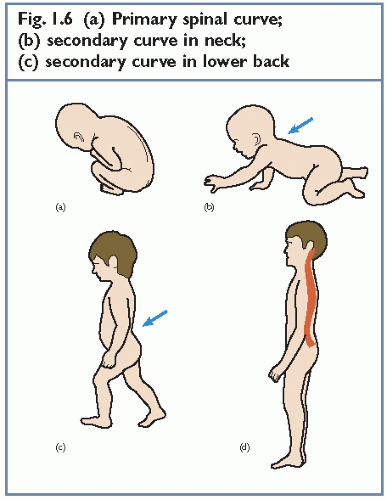 Fig. 1.6 (a) Primary spinal curve; (b) secondary curve in neck; (c) secondary curve in lower back |
If the spine was completely straight, when we run or jump a large amount of shock would be transmitted up to the head. The function of the spinal curves is to enable the spine to act in a spring-like fashion, absorbing some of the shock of movement and making actions more agile.
When the spinal curves are altered, stress can be placed on the spine. This can occur through alterations in posture and the way we work. Long periods spent sitting at desks and driving a car will change the important curve in the lumbar region and this can be one source of low back pain.
Keypoint
Maintaining a correct curve in the lower back is important to overall spinal health.
Another way that spinal curves can change is through exercise. Training one side of the body excessively can lead to an alteration in muscle balance (one muscle being stronger or tighter than another), pulling the spine out of alignment. This is why a balanced exercise programme is so important. The good news, however, is that the spinal curves can often be helped using specific exercises (exercise therapy) – although this can take some time.
The spinal segment
Each pair of spinal bones together forms a single unit called a ‘spinal segment’ (see fig. 1.7). The two bones are separated by a spongy disc attached to the flat part of the bone. At the back of the vertebra the bone is extended to form two small joints called facets. From above, it can be seen that the back of the spinal bone forms a hollow arch through which runs the spinal cord carrying messages from the brain to the legs and arms (see fig. 1.8).
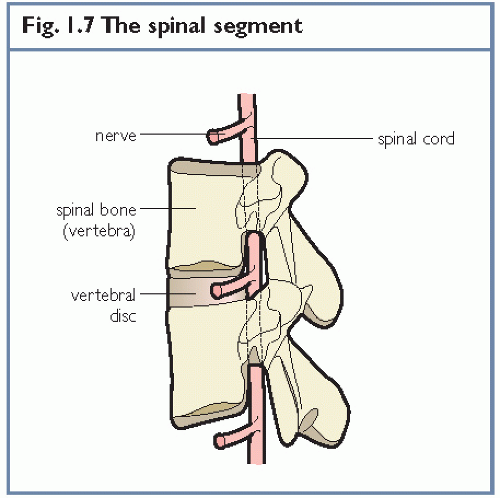 Fig. 1.7 The spinal segment |
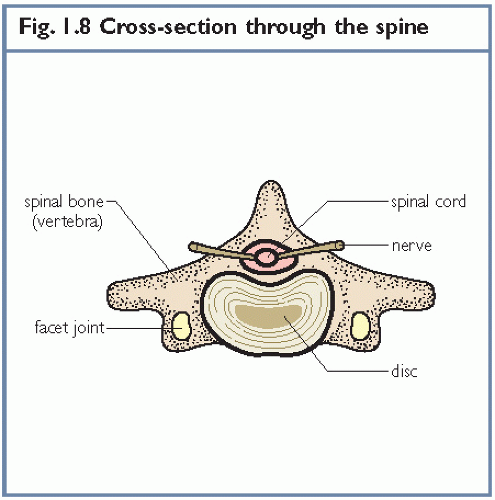 Fig. 1.8 Cross-section through the spine |
Gym users tend to talk about whole spine movements, bending and straightening, often not realising that segments of the spine can move relative to each other. Instructors should look at specific segments of motion, for example, during an overhead shoulder exercise the thoracic spine may be flattening while the lumbar spine may be curving excessively. Therapists look in even closer detail at the individual spinal segments; they are interested in the motion between L5/L4 relative to that of L4/L3, for example. Motion of an individual spinal segment can be important because stiffness in one segment following injury may cause a neighbouring segment to move excessively (compensatory hyper-mobility), causing pain. The answer, here, is to make the stiff segment move more so that the lax segment can move less. A physiotherapist will often use joint manipulation to release a stiff spinal segment and then exercise therapy to re-educate the muscles supporting the lax segment.
Keypoint
Look closer at spinal movements. Notice the movement of (i) the whole spine; (ii) regions of the spine relative to each other; (iii) individual spinal segments.
Spinal ligaments
The spine has numerous ligaments but they broadly fall into two categories. There are those running the length of the spine such as the supraspinous ligament, those running over the top of the spinous processes, and the interspinous ligament, running between the spinous processes. Then there are ligaments associated with individual joints, such as the ligamentum flavum which attaches to the facet joint (see fig. 1.9).
Bending forwards will stretch the ligaments behind the spine but relax those in front. Bending backwards will reverse the situation, stretching the front ligaments but relaxing those covering the back of the spine. Movement of an individual spinal segment will stress the ligaments close to that segment and deep beneath the surface of the body.
If you perform an exercise which persistently overstretches a ligament, the ligament will become sore and inflamed. This may take time to develop so you may not feel pain at the time, but you frequently have backache the next day. If this is the case, change your exercise programme.
If a bent position of the spine is held regularly, perhaps as part of your job, overstretched ligaments will lengthen and those which are relaxed will shorten markedly. This is what happens with poor posture. If you are the sort of person who spends most of their day slumped in
a chair, your spinal ligaments will alter, making it harder for you to hold your spine in a correct alignment when you stand up. To correct this, you must practise exercises to correct your spinal alignment and try to correct your general posture throughout the day.
a chair, your spinal ligaments will alter, making it harder for you to hold your spine in a correct alignment when you stand up. To correct this, you must practise exercises to correct your spinal alignment and try to correct your general posture throughout the day.
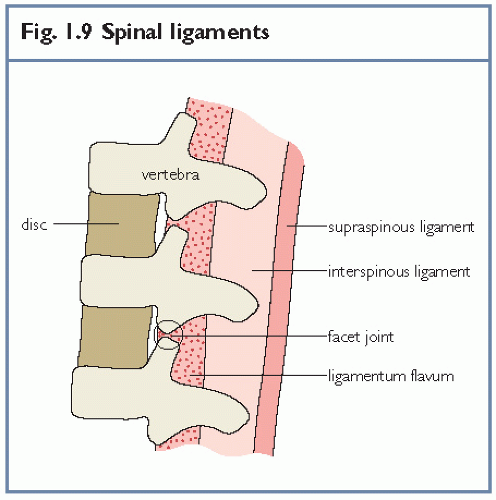 Fig. 1.9 Spinal ligaments |
Keypoint
Repeated bending movements overstretch the spine and can damage it. Cut down on your bending!
Nerves
The spinal cord consists of thousands of tiny nerve fibres bunched together much like a telephone cable. In the same way as the telephone line, the nerves carry electrical messages. When you want to move your leg, for example, an electrical message is sent from the brain. It travels down a nerve contained in your spinal cord to the muscles in your leg, commanding them to move. This is called a motor function.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


