Hand-Assisted Laparoscopic Sigmoid Colectomy
Deborah S. Keller
Harry L. Reynolds Jr.
KEY STEPS
1. Insertion of ports: handport (gelport) midline; 12-mm right lower quadrant; 5-mm suprapubic; 5-mm left lower quadrant (optional for splenic flexure takedown); 5-mm right upper quadrant (optional for inferior mesenteric artery (IMA) ligation).
2. Patient rotated right side down and steep Trendelenburg.
3. Laparoscopic assessment of the abdomen. Hand is used to localize tumor and assess for metastatic disease. Omentum is swept over the colon, and the small bowel is swept out of the pelvis.
4. Lateral-to-medial mobilization along the line of Toldt with identification and avoidance of the gonadal artery and the ureter.
5. Retroperitoneal mobilization of the left colonic mesentery with preservation of Gerota’s fascia.
6. Takedown of the splenic flexure.
7. Medial approach to IMA and inferior mesenteric vein (IMV) with isolation and division.
8. Mobilization of the rectosigmoid junction and the area for transection chosen.
9. Transection of the upper rectum and mesorectum.
10. Exteriorization and resection of the sigmoid via handport.
11. Reinsufflation and anastomosis.
12. Port closure.
ADDITIONAL ADVICE
1. A 30-degree, 5-mm scope allows movement of the laparoscope to any port that can facilitate dissection. Use of additional 5-mm ports may add significantly to exposure with no increase in morbidity.
2. If there is significant inflammation of the sigmoid, the hand is very useful for finger fracturing and opening proper dissection planes. Moving higher along
the descending colon above the area of inflammation may facilitate dissection and allow easier identification of proper planes and the ureter.
the descending colon above the area of inflammation may facilitate dissection and allow easier identification of proper planes and the ureter.
3. If the lateral dissection is difficult, a medial-to-lateral approach as outlined in Chapter 25 with a straight laparoscopic sigmoid colectomy may be used.
4. Full mobilization of the splenic flexure facilitates a tension-free anastomosis and is most easily accomplished prior to exteriorization and resection. It is difficult to tell if the marginal is compromised after resection, anvil placement, and return to the abdomen if additional dissection is required at this point.
5. The assistant holding the omentum anteriorly and cephalad, like a cape, with a grasper placed through a 5-mm right upper quadrant port, facilitates takedown of a difficult splenic flexure. The operating surgeon is between the legs working through a left lower quadrant port and the camera is in the suprapubic port.
6. Division of the IMA at its origin and then division of the IMV just below the pancreas intracoporally facilitate lengthening of the mesentery and a tensionfree anastomosis.
7. In the case of known diverticulitis, an alternative to high ligation of the IMA is to serially divide the sigmoid branches and the left colic, near their origins, with an energy device. This facilitates mesenteric lengthening and a tension-free anastomosis. This avoids the possibility of sympathetic nerve damage.
8. The mesorectum is most easily divided with an energy device taking care to ensure it is divided at a right angle at the level of transection of the rectosigmoid.
9. The descending colonic remnant, with the anvil in situ, should lay easily within the pelvis with the patient in the Trendelenburg position, prior to anastomosis, to ensure it will be tension free.
10. The use of EEA sizers in the rectal remnant prior passage of the stapler helps ensure that there will be limited difficulty in insertion of the stapler to the top of the rectal remnant.
PATIENT POSITIONING
The patient is placed supine on the operating table on a bean bag. After induction of general anesthesia, an oral gastric tube and a Foley catheter are placed. The legs are then placed in yellow fin stirrups in modified lithotomy. Care is taken to ensure the perineum is at the edge of the table to ensure easy passage of the EEA stapler. The legs need to be positioned such that the stirrups can be dropped so that the thighs are at the level of the abdominal wall. If they lay higher, the operator may conflict with the
patient’s thighs while working between the legs taking down the splenic flexure. The arms are tucked. If the patient is too obese to tuck both arms, the left arm is left out as most of the dissection will be on the patient’s right side. The bean bag is aspirated after wrapping it about the shoulders and the patient’s arms.
patient’s thighs while working between the legs taking down the splenic flexure. The arms are tucked. If the patient is too obese to tuck both arms, the left arm is left out as most of the dissection will be on the patient’s right side. The bean bag is aspirated after wrapping it about the shoulders and the patient’s arms.
INSTRUMENT POSITIONING
The primary monitor is placed on the patient’s left side at the level of the shoulder or mid-chest. A secondary monitor is placed near the patient’s right lower abdomen, primarily for the assistant during port placement. The instrument table is placed below the left leg. The nurse stands adjacent to the left leg. The operating surgeon is in the right lower quadrant, with the first assistant to his left, except during port placement. The operating surgeon may move between the legs during splenic flexure mobilization. A second assistant, if available, would stand on the patient’s left side (Fig. 16.1). A 30-degree, 5-mm laparoscope is used.
PORT INSERTION
The applied medical gelport is the preferred handport. A midline incision is made through the umbilicus, and the gelport is inserted (Fig. 16.2). Positioning the incision higher in the abdomen facilitates takedown of the splenic flexure and high
ligation of the inferior mesenteric artery (IMA). Generally, the handport incision length in centimeter corresponds to the surgeon’s glove size or a size smaller. The author wears a size 8 glove, but typically makes a 7-cm handport incision. Any adhesions in the midline are lysed via the port incision. A port is placed through the gelport, and the abdomen is insufflated. A 5-mm suprapubic port is placed. The hand is then placed in the abdomen and a 12-mm right lower quadrant port is placed to allow stapling. An optional 5-mm port is placed in the left lower quadrant to facilitate splenic flexure mobilization. An optional additional 5-mm port in the right midabdomen can be helpful with IMA ligation (Fig. 16.3).
ligation of the inferior mesenteric artery (IMA). Generally, the handport incision length in centimeter corresponds to the surgeon’s glove size or a size smaller. The author wears a size 8 glove, but typically makes a 7-cm handport incision. Any adhesions in the midline are lysed via the port incision. A port is placed through the gelport, and the abdomen is insufflated. A 5-mm suprapubic port is placed. The hand is then placed in the abdomen and a 12-mm right lower quadrant port is placed to allow stapling. An optional 5-mm port is placed in the left lower quadrant to facilitate splenic flexure mobilization. An optional additional 5-mm port in the right midabdomen can be helpful with IMA ligation (Fig. 16.3).
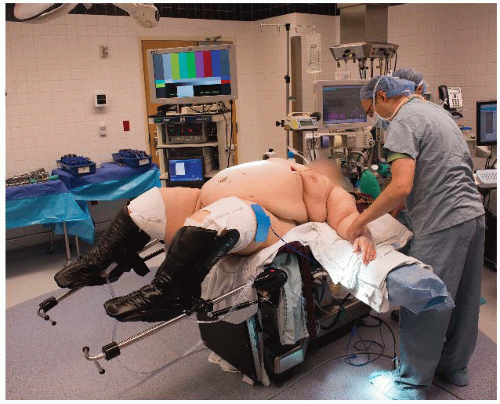 FIGURE 16.1. Room setup. |
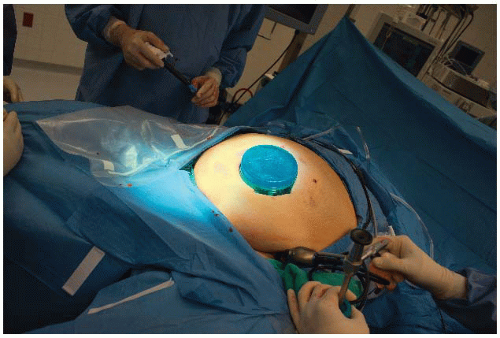 FIGURE 16.2. Insertion of the gelport. |
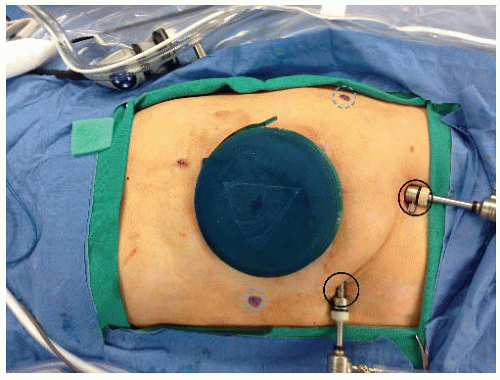 FIGURE 16.3. Port placement. |
The abdomen is insufflated to a pressure of 12 to 15 mmHg and is explored. The liver is examined with the laparoscope and palpated with the hand. The primary tumor is looked at and palpated to determine its location and assess resectability. The remaining abdomen is examined for nodal or peritoneal metastases.
DEFINITIVE LAPAROSCOPIC SETUP
The surgeon begins in the right lower quadrant with the assistant to his left. The camera is in the right lower quadrant port. The surgeon’s left hand is in the abdomen and dissection is initially begun via the suprapubic port. The patient is placed in the steep Trendelenburg position and rotated right side down. The small bowel is swept from the pelvis. The omentum is placed in the upper abdomen cephalad to the transverse colon, overlying the stomach. The orogastric tube placement is confirmed at this time. The hand greatly facilitates these maneuvers. A laparotomy pad can be placed in the abdomen via the gelport. This facilitates packing the small bowel cephalad in obese patients and can also be used to clean the laparoscope periodically without removing the scope from the abdomen.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


